Dry Eye and Ocular Surface Disease Bonus Issue
October 2025
by Liz Hillman
Editorial Co-Director
While this bonus issue of EyeWorld delves into the diverse aspects of dry eye, the Editorial Board thought it was important to call out dry eye masqueraders —conditions that might initially seem like dry eye but aren’t. EyeWorld spoke with Sumitra Khandelwal, MD, to gain insights on these dry eye decoys.
Working at a tertiary care center, Dr. Khandelwal said she sees a lot of people for second and third opinions for dry eye. “There’s a real pattern that I have noticed when it’s not straightforward dry eye,” she said. “It’s not that patients don’t have a component of dry eye—I think we can agree that we all have a little dry eye nowadays with our screen time and environmental changes—but that’s not what is causing them to have symptoms, whether it’s blurry vision or eye pain.”
Source: Stephen Pflugfelder, MD
Dr. Khandelwal said there are several dry eye masqueraders. To identify some of them, she said, it’s important, before putting any drops in the eye, to step back and re-evaluate the comprehensive anterior exam. Look at the lids and lid positioning. “I’ll have patients who have dry eye symptoms … but when you look at it, they have subtle lid positioning issues, and that’s what’s causing some of their symptoms. It’s not necessarily dry eye that needs to be treated with drops,” she said. This could be lagophthalmos, entropy onto the eyelid, or subtle trichiasis. These are things that Dr. Khandelwal said can be missed if the physician goes straight to the slit lamp exam.
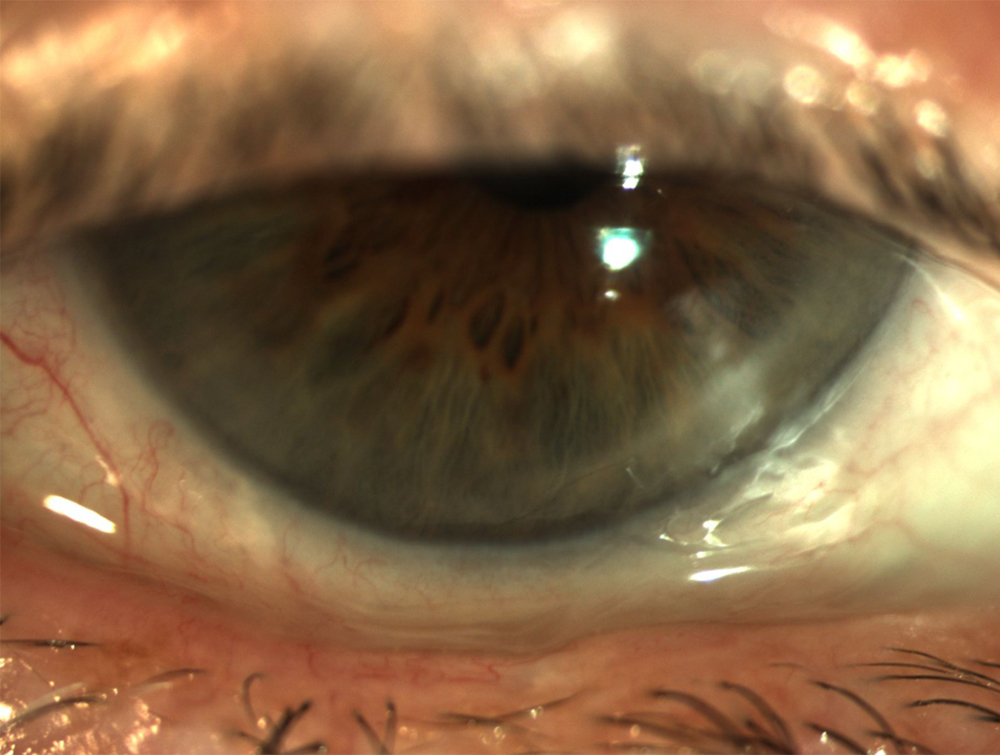
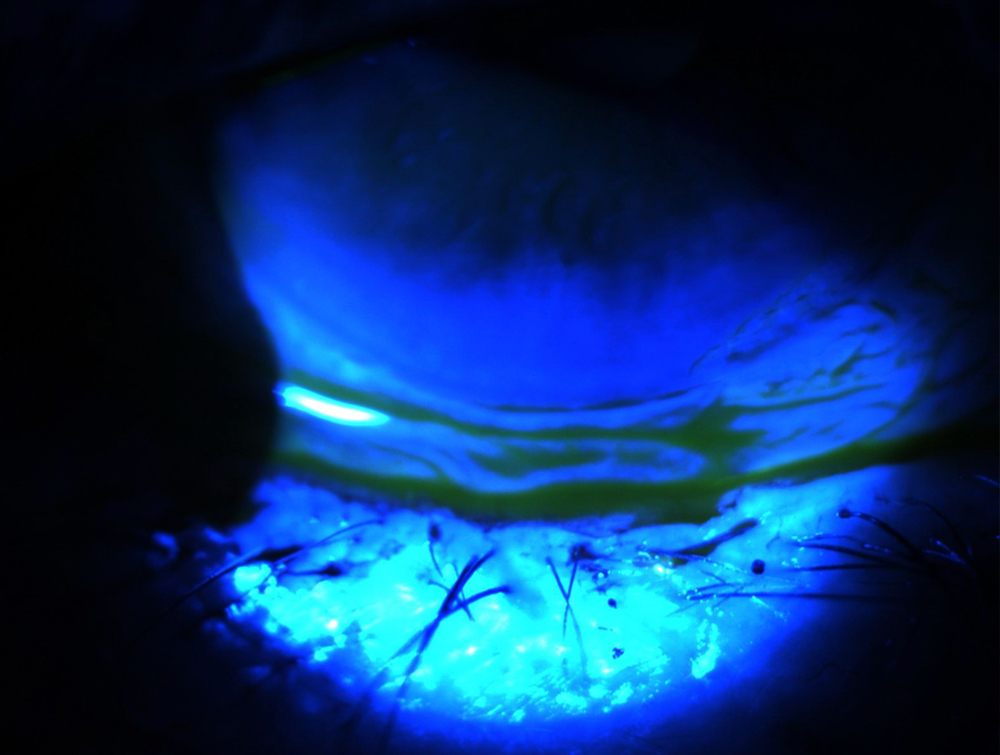
Another item to focus on is the conjunctiva. Dr. Khandelwal said this can reveal conjunctivochalasis, especially on the temporal edges. “When it’s lid issues causing it … you’ll see that the tear film no longer sits correctly. It’s not uniform. So conjunctivochalasis can be a dry eye masquerader.” If you were to try drops in these eyes, they wouldn’t coat the surface; they would sit in the bottom of the conjunctiva and ultimately fall out, Dr. Khandelwal said.
She also said to lift the upper eyelid to look at the superior bulbar conjunctiva. “There are a couple of conditions that we know about from residency but we forget about in real practice. One of them is superior limbic keratoconjunctivitis, also known as SLK. It’s a classic example where there is staining that’s focused on the superior bulbar conjunctiva.” Dr. Khandelwal explained that these patients have more of an inflammatory condition, sometimes with redundancy to the conjunctiva superiorly and occasionally blepharospasm with it. “It’s treated completely differently. Drops only may not help this patient,” Dr. Khandelwal said, explaining that they typically need an anti-inflammatory, an immunomodulator, cauterization, and/or botulinum toxin A to help with the blepharospasm.
Other dry eye masqueraders include Demodex and staph blepharoconjunctivitis. “If patients have a lot of staph and have ocular rosacea on their eyelids, if they have Demodex collarettes, they need to be treated differently than your typical dry eye patient.”
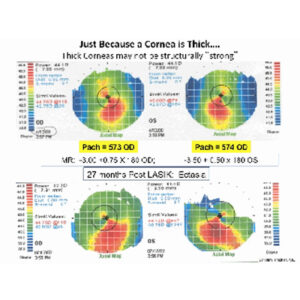
Salzmann’s nodules or epithelial basement membrane dystrophy can masquerade as dry eye on Placido topography as well. “The epithelial basement membrane dystrophy can be very subtle. It can present with negative staining, instead of just frank cysts and map-dot. You want to look at that and match it up with the topography to understand if the patient’s symptoms are something on the ocular surface. It could be from these little hills and valleys that have developed over the years, and they would need superficial keratectomy if typical medical management doesn’t work.”
Neurotrophic keratitis is another condition that is frequently mischaracterized. “It’s easy to say the patient has dry eye, but in reality, the neurotrophic keratitis patient has more of a lack of reactive reflex tearing and loss of their typical immunomodulators that are in the tear film,” Dr. Khandelwal said. Sometimes they get better with dry eye treatment, but sometimes they plateau. When patients continue to have a lot of staining despite treatment, it’s important to check their corneal sensation.

Source: Stephen Pflugfelder, MD
Awareness of neurotrophic keratitis is on the rise due to an increase in education and because there are treatment options. “I think for any patient who comes in and the staining pattern on their cornea is more than their symptoms—it’s staining without pain or staining with minimal pain—to me, that’s a red flag they have neurotrophic keratitis,” Dr. Khandelwal said, adding that if their Placido disc topography looks suspicious, it is a stopping point for technicians to not put drops in their eye. If drops have already been put in the patient’s eye, Dr. Khandelwal said she asks the patient if their eyes often feel dry. If they say their eyes ache every now and then, she’ll check corneal sensation upon their arrival next time prior to any drops.
Some inflammatory conditions, Dr. Khandelwal noted, can overlap with dry eye but are more significant than “just dry eye.” Other conditions that are more than “just dry eye” include things like limbal stem cell deficiency and ocular cicatricial pemphigoid. Limbal stem cell deficiency can present as a few clock hours of superiorly or subtle corneal neovascularization and a whorl-like staining pattern. Many of these patients are long-time contact lens wearers who have focal limbal stem cell deficiency. Patients with cicatricial pemphigoid often present late, but Dr. Khandelwal said ocular symptoms start somewhere.
“If I see a patient in the clinic who has dry eye and hasn’t gotten better, and they have some little focal areas where there’s a thickening to the conjunctiva and maybe even a little early symblepharon formation, I do a conjunctival biopsy. If that comes back with a loss of goblet cells, it is just ocular surface disease. But I’ve had several patients through the years who have early ocular cicatricial pemphigoid. It’s got a classic pathology with immunofluorescence staining,” she said.
These tips can help providers to remember not all dryness is dry eye. Watch out for these masqueraders, and always keep them on your differential for a patient not improving with typical ocular surface treatment, Dr. Khandelwal said.
About the physician
Sumitra Khandelwal, MD
Professor
Department of Ophthalmology
Baylor College of Medicine
Houston, Texas
Relevant disclosures
Khandelwal: AbbVie, Dompe
Contact
Khandelwal: Sumitra.Khandelwal@bcm.edu