Refractive
Spring 2026
by Ellen Stodola
Editorial Co-Director
The management of astigmatism is crucial to achieve the best outcomes possible for cataract surgery, said Eric Donnenfeld, MD, who finds that he has “zero tolerance” for astigmatism. “I think all levels of cylinders should be treated as best as possible.”
Dr. Donnenfeld and Rahul Tonk, MD, MBA, shared their thoughts on the various ways to manage astigmatism, what levels to treat, and how they decide the best option for each patient.
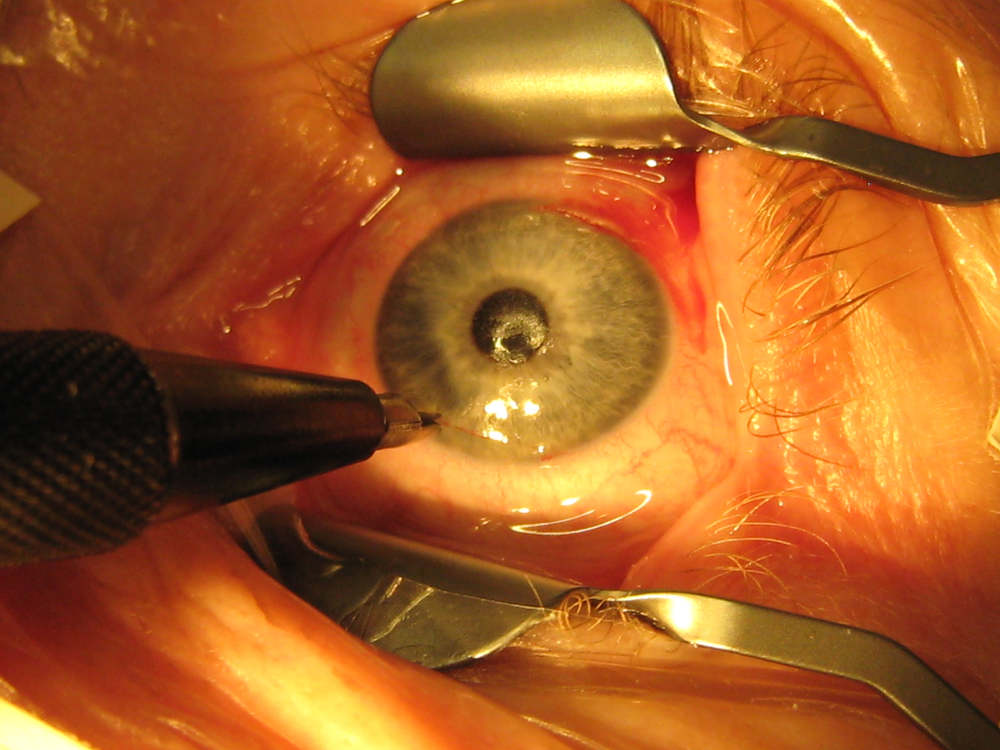
Source: Eric Donnenfeld, MD
Dr. Donnenfeld noted that there are several different ways of managing astigmatism. For low levels, you can do on-axis incisions. You can do cataract surgery and put your incision at the axis of the cylinder, and if you feel comfortable doing that, it’s a very reasonable thing to do, Dr. Donnenfeld said.
For very low levels of astigmatism, Dr. Donnenfeld recommended a relaxing incision, particularly for 0.5 D or 0.75 D or less. That’s an easy procedure to perform, he said. “It could be done with a diamond knife, but I’m now doing most of my relaxing incisions with what I call a penetrating relaxing incision,” he said. “I’m taking a keratome and making a full thickness, beveled incision at the axis of the cylinder after taking into account the posterior corneal cylinder and the induced astigmatism from the phaco incision,” adding that the nice thing is that everyone is accustomed to that.
The femtosecond laser can also be used for relaxing incisions, particularly for those who don’t feel comfortable doing diamond knife incisions. The laser helps make a reliable incision at the correct depth, he said, and newer laser platforms can incorporate the patient’s preoperative keratometry, the posterior cornea, and the surgically induced cylinder to use vector analysis to make sure that the limbal relaxing incision is done in the right place. He added that the Donnenfeld nomogram was incorporated into the CATALYS laser (Johnson & Johnson Vision), so it’s also automatically a tool to treat cylinder.
Dr. Tonk categorizes his options for treating astigmatism into four tools: toric IOLs (monofocal and presbyopia-correcting), the Light Adjustable Lens (LAL, RxSight), femtosecond arcuate keratotomy (FSAK), and manual limbal relaxing incisions (LRI).
“My clinical algorithm splits patients into ‘low’ versus ‘moderate-to-high’ astigmatism,” he said. “For low amounts of cylinder (typically <1.0 D), I lean toward corneal relaxing incisions (FSAK/LRI). For moderate-to-high astigmatism, I prefer an implant-based solution (toric IOL) due to superior stability and predictability.”
When discussing these options with patients, Dr. Tonk said he will avoid getting into the weeds of the specific tools. “I use the analogy of commissioning an artist: When you hire a painter, you don’t ask them what specific brush or pigment they are using; you care about the final portrait,” he said. “Similarly, I tell patients my goal is to deliver the clearest possible image, and I will select the specific tool (laser, toric lens, or adjustable lens) that best achieves that result for their unique eye.”
Dr. Donnenfeld finds that patients are very receptive to options for treating astigmatism. “I say to them, ‘You have astigmatism, we have two different options, and I think in your case, this is the best option.’”
For higher levels of astigmatism, Dr. Donnenfeld likes the option of using a toric IOL, and when given the opportunity to choose between a toric or relaxing incision, he will pick a toric.
There are some toric IOLs to treat lower levels of astigmatism, down to 0.7 D, he said, adding that Bausch + Lomb has one for 0.75 D. Those are the go-to lenses for Dr. Donnenfeld for higher levels of astigmatism. “I think that they are tremendously underutilized,” he said. “About 50% of patients have 0.75 D or more cylinder, so I think toric lenses are the entry point for most doctors in doing refractive cataract surgery. I often get asked, ‘How do you get started in refractive cataract surgery?’ and I say, ‘Don’t start with a multifocal IOL; start with the toric IOL.’ That’s the low-hanging fruit for managing these patients, and I think we should do a lot more of that.”
There may be some cases where you’re unsure how to proceed, predominantly patients who are post-LASIK and have cylinder or those with underlying problems that make it less likely that you’re going to hit the nail on the head. You can always manage cylinder with an LAL. That’s a good way of managing cylinder when you don’t feel confident in a toric IOL, he said.
Dr. Tonk also prefers to use toric IOLs when possible, and he also likes to treat all astigmatism. However, he noted that a “gap” exists in current inventory because most platforms start at around 1.25–1.50 D at the IOL plane. “Consequently, I generally select toric IOLs only when corneal astigmatism exceeds 0.75 D (against-the-rule) or 1.0–1.25 D (with-the-rule).”
For patients falling into this gap, where a toric is too powerful but the astigmatism remains visually significant, Dr. Tonk said he relies on FSAK or the LAL.
Toric IOLs, he said, offer the highest predictability and stability for significant astigmatism, but they are fixed. “If the effective lens position varies or the lens rotates, the result is compromised.”
Meanwhile, he said that corneal incisions (FSAK/LRI) are less invasive in terms of hardware but less predictable for higher magnitudes of correction. “They also carry a risk of regression over time and can exacerbate dry eye symptoms by severing corneal nerves.”
Dr. Tonk said the LAL has become a “problem solver” for predictability. “It allows us to treat residual refractive error postoperatively, essentially eliminating the variables of effective lens position and healing response.”
The decision on which lens to choose is often more of an issue of the patient’s visual request rather than the cylinder, Dr. Donnenfeld said. “I do about 70% of my cases with a monofocal or a monofocal plus lens, and I do about 30% with a multifocal lens,” he said. Additionally, as EDOF lenses become better—with new options expected this year—he thinks there will be more of an uptick in use of these options.
“I think we’ll be doing more EDOF toric lenses as well,” he said, adding that it’s an easy conversion to go from a multifocal to an EDOF lens. “They don’t get quite as much reading, but their quality of vision is much better at distance.”
Postoperatively, when you’ve done cataract surgery and there is still residual cylinder, Dr. Donnenfeld said a slit lamp limbal relaxing incision can be a good option to manage these patients.
Dr. Tonk said he views this choice between lens options as a hierarchy, with the base being ocular health. “If the macula, optic nerve, or ocular surface are compromised, I steer away from presbyopia-correcting options,” he said. “If the ocular health is pristine, we move to the next layer: lifestyle. I ask myself, ‘Would this patient have a richer life without the burden of glasses and contacts? What are their specific visual tasks, and how do they use their eyes?’ The final layer is preference, specifically their willingness to accept potential optical imperfections or photic phenomena in exchange for spectacle independence.”
Dr. Tonk said that certain levels of astigmatism make certain lenses more desirable. Presbyopia-correcting IOLs (especially diffractive multifocals) are less forgiving of residual astigmatism than monofocals. “Even small amounts of residual cylinder can significantly degrade the modulation transfer function and image quality in a multifocal eye,” he said.
Dr. Tonk added that if a patient has irregular astigmatism or a level of cylinder where he cannot guarantee a residual <0.50 D, he will generally avoid diffractive PC IOLs. “In these cases, the LAL is an excellent alternative, or I stick to a monofocal toric to ensure quality of vision over range,” he said.
About the physicians
Eric Donnenfeld, MD
Clinical Professor of Ophthalmology
New York University
Ophthalmic Consultants of
Long Island
Garden City, New York
Rahul Tonk, MD, MBA
Cornea, Cataract, and Refractive Surgeon
Princeton Eye Group
Associate Professor of Ophthalmology
Wills Eye Hospital
Princeton, New Jersey
Relevant disclosures
Donnenfeld: Alcon, Bausch + Lomb, Johnson & Johnson Vision
Tonk: None
Contact
Donnenfeld: ericdonnenfeld@gmail.com
Tonk: rahul.tonk@gmail.com


