Cornea
Spring 2026
by Ellen Stodola
Editorial Co-Director
Epithelial basement membrane dystrophy (EBMD) is a common corneal issue. Winston Chamberlain, MD, PhD, and Christopher J. Rapuano, MD, discussed how this might present in patients and the number of treatment options available to address the condition, with surgeons often needing to use several different strategies.
EBMD causes a couple of main problems, Dr. Rapuano said. The first is it can cause irregularity to the surface of the cornea and distort vision. It’s less common that it does this than the recurrent erosion, he said, but it’s still important to realize that EBMD can cause patients to have decreased vision, and they’ll often call it “shadow vision” or “double vision.” When someone comes in complaining of double vision, Dr. Rapuano said the first thing to do is figure out if it’s with both eyes open, which means their eyes aren’t aligned properly, or if it’s with one eye open, in which case it’s often a cornea problem, like EBMD.
The best way to test for EBMD is by putting fluorescein in and looking for negative staining, he said, which is where the fluorescein runs off the high points in the cornea, and “these little mountaintops stick out, and that causes the distortion of the vision.” If you look hard enough, many patients have mild, typically peripheral, asymptomatic EBMD changes, but it is still important to know in case they develop symptoms in the future. Most of the time EBMD won’t cause visual problems.
EBMD can also cause recurrent erosion problems, he said, and that’s because the irregular layer of epithelial cells is not cemented properly to the cornea. If it gets very loose or is so loose it comes off, it causes recurrent erosions.
Dr. Rapuano said the main symptoms of recurrent erosions range from mild foreign body sensation and short periods of pain to long periods of pain, typically either in the middle of the night or when people wake up in the morning. “We think that’s because the eyes are closed overnight, and they tend to dry out, so the eyelid sticks to the surface of the cornea and pulls off this loose epithelium,” he said.
Sometimes the patient has mild pain when they wake up in the morning, but the EBMD changes can often be hard to see upon exam, Dr. Rapuano said. Other times, it may be more obvious or it looks like a large corneal abrasion. It’s important to look at the other eye because sometimes in the “normal eye,” you’ll see the EBMD changes, and in the bad eye, you’ll see a big scratch and very loose epithelium, and you’re not sure why it’s there.
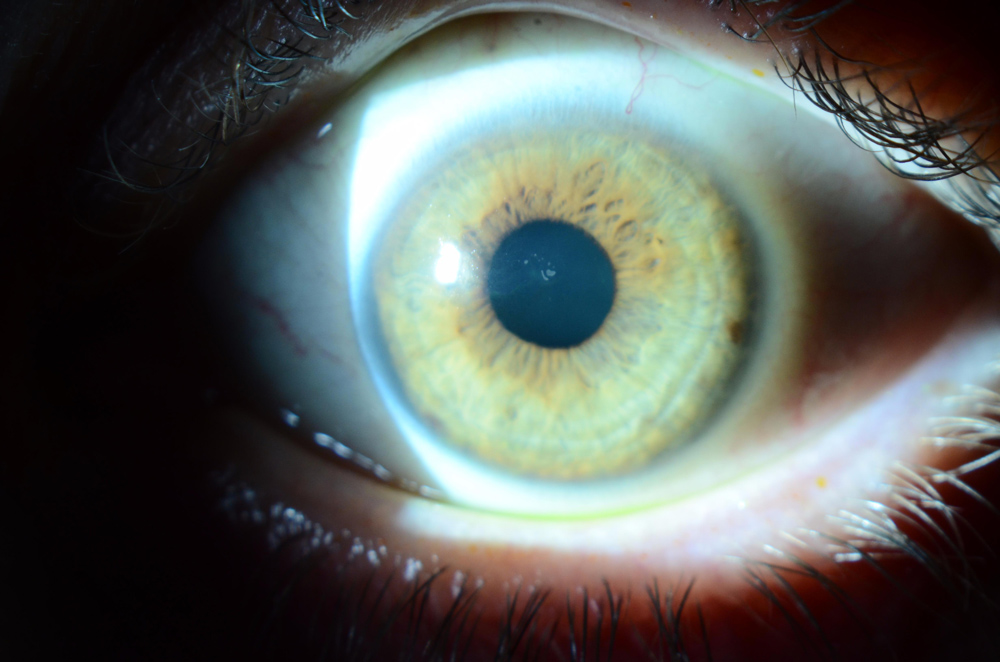
Source: Christopher J. Rapuano, MD
Early treatment options
For treatment options, Dr. Rapuano said it depends on how bad the symptoms and exam findings are, and he often takes a stepwise approach. If they have a large corneal abrasion, you need to treat it with antibiotics to prevent an infection, he said. If the patient is in a lot of pain or has a bad epithelial defect, a bandage contact lens can be used temporarily with antibiotic coverage.
If the epithelium is sloughing off or is so loose that it’s barely hanging on, you can do an epithelial debridement, Dr. Rapuano said. This helps to remove all the non-adherent epithelium. Sometimes you can use a pressure patch, but usually either antibiotic ointment or a bandage lens will help the patient heal. If you can get them to heal, you want to then use preventative treatments to keep it from coming back.
To prevent this from recurring, keep the eye lubricated during the day, but the key thing is to use some type of lubricating or antibiotic ointment at night. This involves ointment/gel between the eyelid and the eyeball so that the eyelid can’t pull on the loose epithelium. Over weeks to many months, Dr. Rapuano said, the epithelium lays down its proper cement, and ideally it doesn’t happen again. He recommends using ointment every night for 6 months, including if taking a nap. While these instructions are simple, the routine can still be challenging.
If this preventive treatment doesn’t work, Dr. Rapuano said there are other options. One option is a bandage soft contact lens that you put in the eye for about 6 months, replacing every month or two. The disadvantage of that is the extended wear does increase the chance of infection, he said, adding that infection may cause significant scarring.
Dr. Chamberlain also noted the many conservative treatment options to start these patients on, beginning with topical lubrication and nighttime ointments, including hypertonic saline ointment, bandage soft contact lens therapy, topical antibiotics to prevent infection in overt epithelial breakdown, and oral antibiotics such as doxycycline and tetracycline, which may reduce matrix metalloproteinase activity. Other available options might include autologous serum drops, amniotic membranes, and careful use of low potency topical corticosteroids, he said, which may also reduce inflammation associated with and causative of erosions.
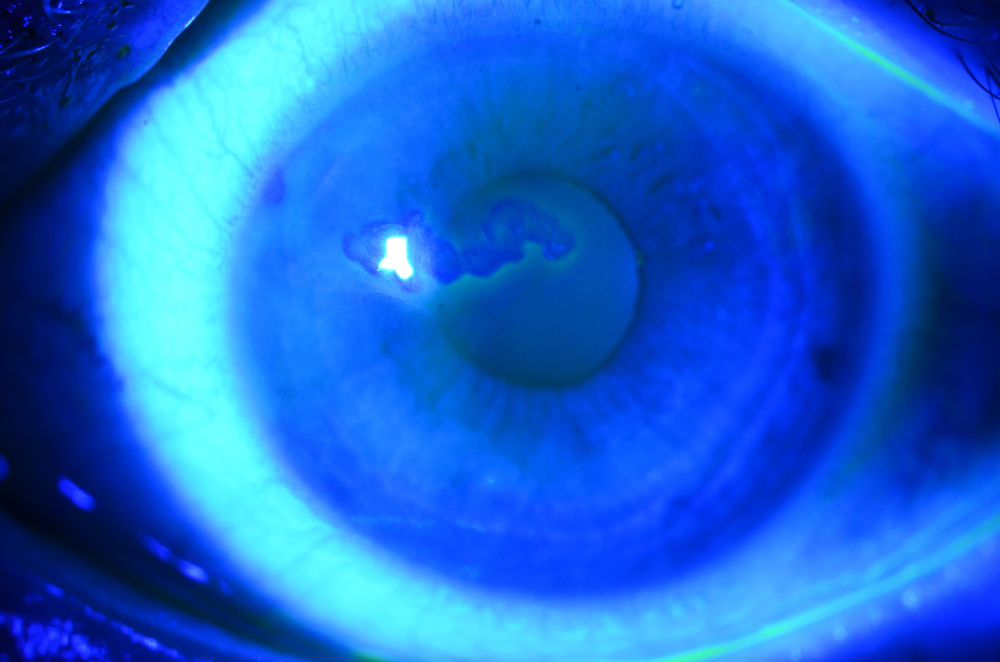
Source: Christopher J. Rapuano, MD
Advanced treatment options
When conservative treatment options fail, as Dr. Chamberlain noted they do in more than 50% of cases, surgical options include superficial keratectomy with diamond burr polishing (DBP), anterior stromal puncture (ASP), alcohol delamination/removal of epithelium, and excimer laser phototherapeutic keratectomy (PTK).
ASP creates focal stromal scars using a bent needle to enhance epithelial adhesion, he said, adding that the PTK approach uses excimer laser ablation to remove abnormal basement membrane and create a smooth surface for epithelial regeneration.
Treatment for EBMD and recurrent corneal erosions typically begins with conservative measures and escalates to surgical interventions when medical therapy fails, Dr. Chamberlain stressed. He added that treatment choice depends on lesion location, severity, recurrence pattern, and prior treatment response, with some patients requiring repeated or combination therapies to achieve optimal outcomes.
Off-center zones of erosions may respond to stromal puncture, while central zones often benefit more from superficial keratectomy with burr or PTK.
Dr. Rapuano said he will often use diamond burr polishing, for which he gives the patient numbing drops and uses a blade to remove all the loose epithelium anywhere that looks irregular. “As opposed to those with post-traumatic recurrent erosions, for patients with EBMD, it’s usually the entire cornea,” he said. Even though they’ve only had an erosion in one area, it tends to be loose everywhere. Dr. Rapuano will debride the epithelium to the limbus and use a 5-millimeter diameter fine-grit diamond dusted burr, going over the entire cornea for about 5–10 seconds. The idea is that it’s removing any kind of residual basement membrane that’s abnormal in these EBMD patients, he said. Post-treatment, Dr. Rapuano will use a bandage soft contact lens and antibiotic drops.
The other option, he said, is excimer laser PTK, which is an identical treatment except instead of the diamond burr, you use a laser to smooth out the surface.
When doing PTK, Dr. Rapuano said you only need to remove 5 or 6 microns of tissue in any particular location. Downsides to the laser are not everyone has one, and it’s more expensive. Additionally, the laser diameter is usually not the entire cornea, so you have to use multiple spots. “You don’t want the spots to overlap, so it’s a little trickier to do,” he said.
Stromal puncture, Dr. Rapuano said, is another good treatment, but it’s usually not great for patients with EBMD because eyes with EBMD tend to have more diffuse pathology where the entire epithelium is abnormal and loose. It also requires diffuse treatment, including in the visual axis.
“Where ASP works well is in post-traumatic recurrent erosions,” he said. “Let’s say someone gets poked in the eye. It’s just a small abnormal area, where they were poked. The rest of the epithelium is totally normal. All the erosions are in the exact same area. Then I’ll do stromal puncture, as long as the abnormal area is relatively small and also not in the visual axis.” Dr. Rapuano added that he doesn’t like to do punctures in the visual axis because the punctures leave small scars. When doing a stromal puncture, he uses a 25-gauge needle and will treat anywhere from 50 to several hundred spots, as close together as he can.
Both PTK and ASP are effective, but each has advantages depending on clinical context, Dr. Chamberlain said. “PTK requires excimer laser expertise and access to the laser equipment with associated costs,” he said. “It may be better for central lesions than ASP.” He added that PTK can shift the refraction in the eye and typically would induce a hyperopic shift, which may not be desirable. “But this might provide an added advantage on slightly myopic patients to reduce refractive error.”
Meanwhile, he said that ASP is a simpler office-based procedure, requiring only a bent small-gauge needle and slit lamp proficiency. The size of the barb or bend on the needle should be quite small to reduce significant stromal scarring, which can induce irregular astigmatism and focal opacities in the cornea, Dr. Chamberlain said, but a higher level of scarring may produce better epithelial adherence.
Success rates are comparable with PTK, ASP, and superficial keratectomy with diamond dusted burr. “Various studies report different rates,” Dr. Chamberlain said. “I usually quote about a 70–80% success rate across all treatments after first treatment with some reduction in success rates with sequential treatments.”
Dr. Rapuano said techniques for EBMD and recurrent erosions are easy for any ophthalmologist to learn. Diamond burr polishing is pretty straightforward, he said. “You can watch a video online and know what to do,” he said. “The key is to only treat the cornea for about 10 seconds.” Stromal puncture is a little trickier because you’re taking a needle to someone’s cornea, but any proficient ophthalmic surgeon should be able to do that. He added that you want to be careful not to perforate. He said to make sure the patient’s forehead is firmly up against the headband while you are performing the procedure—you don’t want to be moving forward at the same time they are.
With PTK, Dr. Rapuano said, there’s a certain skillset that goes along with that, but it’s not too difficult. With PTK, however, he warned not to go too deep. “I’ve certainly seen many doctors go too deep, and that causes more haze and a refractive error,” he said.
Some patients require repeated or combination therapies to achieve optimal outcomes, Dr. Chamberlain said. Superficial keratectomy with diamond dusted burr can occasionally leave a few zones that need spot retreatments. “If a focal zone of recurrence is found, a focal repeat scraping and burr can be applied.” Meanwhile, he said that repeated failures merit trial of alternative therapies, particularly if zones of loose epithelium are large. Failure may also benefit from prolonged use of the oral and topical treatments that can help the epithelium heal with better hemidesmosome (basement membrane anchors) formation.
Additional considerations
Dr. Rapuano added that some patients will benefit from a medical treatment, along with topical steroid drops for a month or two, though he hasn’t found this approach to be very helpful. He also said to make sure you’re treating any other ocular surface conditions that may be going on, particularly if the patient has dry eye, blepharitis, or Demodex.
Dr. Chamberlain added that well-designed randomized, controlled trials are needed to establish definitive treatment guidelines. A Cochrane review found that existing studies are of insufficient size and quality to provide firm evidence for management protocols.1 International consensus on standardized outcome measures and approaches could improve outcomes, he added.
Article Sidebar
Plexitome device for stromal puncture
The Plexitome (VEO Ophthalmics) is a new device that may do a better job at anterior stromal puncture than a bent small-gauge needle, Dr. Chamberlain said. “It is a microfabricated disposable (one-time use) instrument recently approved for anterior stromal puncture that allows the ophthalmologist to safely perform stromal puncture in the optical axis,” he said. “The Plexitome’s ability to create micropunctures without visible scarring potentially expands the utility of stromal puncture to central lesions, offering a simpler, office-based alternative to laser procedures or the more invasive scraping and diamond dusted burr.” He noted that there is not yet long-term data or a sense of where it fits into the treatment algorithm.
Article Sidebar
ASCRS Annual Meeting Preview
John Hovanesian, MD, EyeWorld Cornea Editorial Board member, shared what he is looking forward to at the 2026 ASCRS Annual Meeting:
“Every year, what I look forward to most at the ASCRS Annual Meeting is seeing the great people, new and old friends, who make this meeting so collaborative and fun. There’s no meeting that brings together more refractive and cataract surgery-focused colleagues for an intense period of learning and sharing. I will never miss an ASCRS Annual Meeting.”
About the physicians
Winston Chamberlain, MD, PhD
Affiliate Professor of Ophthalmology
Northwest Permanente, P.C.
Casey Eye Institute
Oregon Health & Science University
Portland, Oregon
Christopher J. Rapuano, MD
Chief of the Cornea Service
Wills Eye Hospital
Professor
Sidney Kimmel Medical College
Thomas Jefferson University
Philadelphia, Pennsylvania
Reference
- Watson SL, Leung V. Interventions for recurrent corneal erosions. Cochrane Database Syst Rev. 2018;7:CD001861.
Relevant disclosures
Chamberlain: None
Rapuano: None
Contact
Chamberlain: chamberw@ohsu.edu
Rapuano: cjrapuano@willseye.org


