Refractive: Opening doors
Winter 2025
by Liz Hillman
Editorial Co-Director
Dysfunctional lens syndrome (DLS) has evolved from a theoretical framework to a clinically validated tool that’s reshaping patient education and surgical decision making. Described over a decade ago, the dysfunctional lens staging system now plays a role in identifying the right intervention at the right time—particularly in the growing field of custom lens replacement.
DLS background
The term dysfunctional lens syndrome was coined by George Waring IV, MD, Jason Stahl, MD, and Daniel Durrie, MD, around the concept of optical lens dysfunction originally proposed by Jorge Alió, MD, PhD.1 Dr. Alió and colleagues described for the first time the evolution of the density and of the anterior and posterior nucleus, and MTF value using an optical quality analysis system from 8–80 years of age finding their association over a person’s life. This was the basis of the theory of dysfunctional lens syndrome.
The early concept, Dr. Waring said, described early opacification of the human crystalline lens. “We knew the other aspects of crystalline lens aging such as presbyopia and higher order aberrations were also important and could be characterized, in addition to lens opacification, in a syndromic term.”
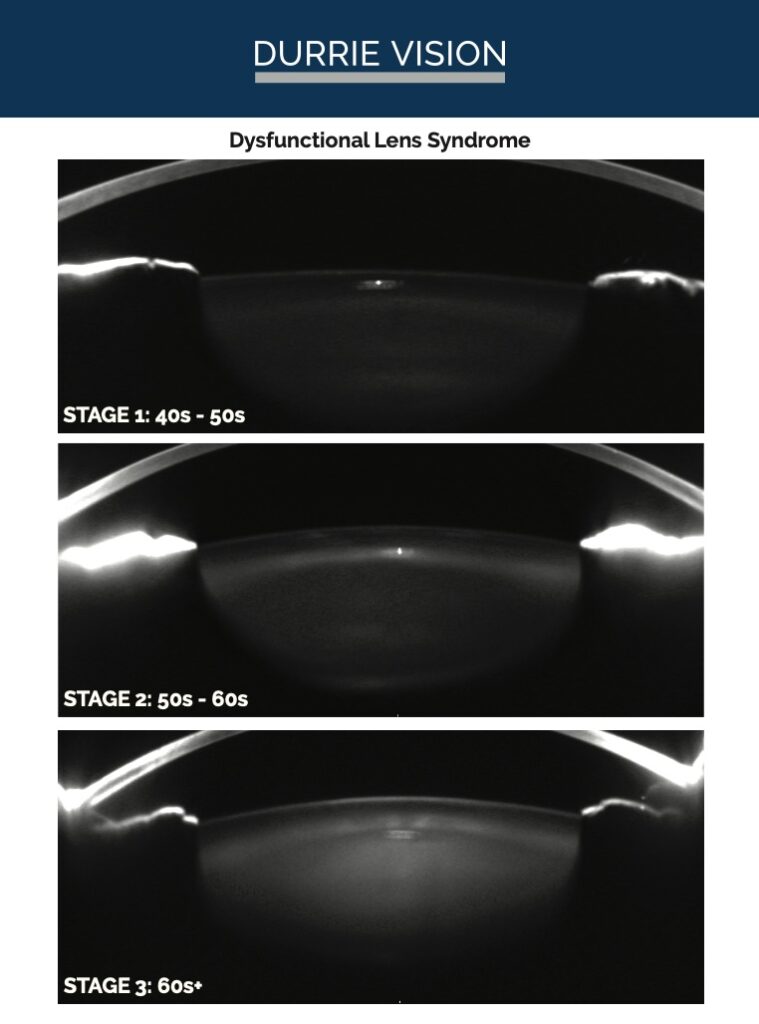
Through the years, Dr. Waring recounted, they proposed a system of staging, with Stage 1 being presbyopia, Stage 2 being presbyopia, increased aberrations, and early opacification, and Stage 3—the final stage—being a manifest cataract that consistently adversely affected daily activities.
Over time, published research increased, and a scientific basis for lens dysfunction and its various stages was established. Dr. Waring said the staging system became useful for surgical decision making and for patient education.
“One of the main reasons that we set out to study and better characterize this was the standard of care for vision correction was LASIK in the dysfunctional lens cycle. We realized a phenomenon over and over where we may have performed LASIK in patients and they’d come back a number of years later saying, ‘My LASIK wore off.’ We all knew that wasn’t true. We learned that the internal lens had become dysfunctional, hence the opportunity for scientific study and validation.”
Source: Jason Stahl, MD
DLS as a patient education tool
Dr. Waring said that, over time, dysfunctional lens syndrome staging and related diagnostic and imaging equipment has helped patients better understand the need for refractive lens exchange/custom lens replacement. “When we would talk about lens replacement, [patients] were unsettled and, because this was a foreign concept to them, would often go elsewhere seeking LASIK. They just were not comfortable with this idea … but we knew that it was the right thing to do because if we’re going to fix something, we want to go to the source of the problem, and we had a scientific basis for this as well. Showing the additional opportunities for lens replacement, based on our research, we were able to demonstrate not only improvement in uncorrected visual acuity for distance but also improvement in other objective measures, qualitative measures, to improve quality of vision,” Dr. Waring said. “This is where the tables started to turn. We could fix things that we couldn’t fix with LASIK with lens replacement. As the terminology became progressively adopted by the medical community, we also saw the adoption start to increase.”
In the early 2000s when patients who were initially happy with their LASIK were coming back to say it had worn off, there was not the diagnostic technology to show what was actually happening, Dr. Stahl said. “You can explain to them that it’s the lens. Then they ask, ‘Do I have a cataract?’ It’s not a cataract, but it’s dysfunctional. So that’s where we came up with dysfunctional lens syndrome, and we started to characterize the different stages. What made our discussion easier was the development of new diagnostics that could actually show the patient their lens and describe what’s happening and why this is going to continue to be an issue in the future.”
Dr. Stahl said he has found the Pentacam (Oculus) densitometry image of the patient’s lens to be helpful from an educational standpoint. “You can show them the lens scatter,” he said, and compare that to the scatter with Stage 1, Stage 2, and Stage 3 dysfunctional lens syndrome.
“Showing them that and next a color slit lamp image of their lens, you can show them that there’s some scatter, there’s some yellowing,” he said.
Dr. Waring said due to an increase in public education, the pendulum has swung to the point where patients are coming in requesting custom lens replacement but are having to be recommended LASIK because they’re not yet candidates. “Previously, we would turn them away for LASIK and recommend custom lens replacement. Now we have people coming in asking for custom lens replacement, but we’re actually not recommending it,” he said.
Refining the DLS nomogram
Since dysfunctional lens syndrome was originally proposed more than a decade ago, the nomogram for treating it has evolved dramatically, Dr. Waring said.
“Like everything else in medicine, usually it starts in the most severe phases, and as the technology improves, the research improves, the innovation improves, and our confidence to deliver improves, the intervention moves further along earlier in the intervention cycle. That’s exactly what we’ve observed with custom lens replacement,” Dr. Waring said.
When the DLS nomogram was originally conceived, corneal vision correction might have been recommended for the surgical correction of pure presbyopia. Dr. Waring said that now, more often than not, for patients who are plano presbyopes (J6 or worse), he’s recommending custom lens replacement. “They still have great distance. They still have excellent quality of vision. They may be better than perfect uncorrected, but they are fully dependent on reading glasses for everything that they do and are looking for a solution for their reading vision, so in the appropriate patient, we’ve moved to custom lens replacement as our primary procedure in the first stage of lens dysfunction.”
The innovations that have led to confidence in recommending custom lens replacement at earlier stages of dysfunctional lens syndrome include presbyopia-correcting IOLs that have improved contrast sensitivity and optical quality, as well as full range of vision lenses, Dr. Waring said. Dr. Stahl said diagnostics that allow the surgeon to show the patient what’s going on with their lens have been pivotal as well. In addition, the use of the femtosecond laser in custom lens replacement provides a LASIK-like experience, Dr. Waring added. “We’re still providing a laser eye procedure with a femtosecond laser. … But custom lens replacement has additional benefits and features: 1) it goes to the source of the problem and 2) we keep both eyes balanced, both eyes seeing distance and near. … Custom lens replacement is designed to not only improve upon the distance vision but also restore the reading. … Custom lens replacement is enduring, it’s anti-aging, it prevents the eventual aging changes and prevents the necessity for cataract surgery.”
Even with all the benefits of custom lens replacement for patients with dysfunctional lens syndrome, Dr. Waring said it’s important to remember that, as with all procedures, not everyone is a candidate. “On occasion we see the “in-betweeners,” who might not be an ideal candidate for anything, and we recommend no surgery. The good news is with advanced technology and advanced diagnostics, many people are a candidate.”
Dr. Stahl said his DLS nomogram comes down to what he sees on the evaluation and where the patient says they’re struggling with their vision. If the patient is 20–44, he or she is a candidate for laser vision correction or the EVO ICL (STAAR Surgical) in his practice. There’s the rare 35-year-old who is a +5 hyperope and, if they’re experiencing reading issues, could be a candidate for refractive lens exchange, but usually these patients are advised to wait until they’re in their 40s and officially in Stage 1 DLS.
The 45- to 50-year-old patient is interesting, according to Dr. Stahl, because 10 years ago, he would have done LASIK on these patients, especially if they were myopic. Now he’s talking to them about refractive lens exchange. “We tried doing LASIK in these patients years ago, and they’re happy initially but then they come back in a few years as they continue to lose more accommodation.”
If the patient is a low myope in their 40s with decent accommodation, Dr. Stahl said they could be a candidate for LASIK with a slight blend. He said he is sure to explain to these patients that they are “kicking the reading glasses can down the road.” If this and future distance vision changes might upset them, they should consider refractive lens exchange.
Dr. Alió said due to the risk of retinal detachment in myopes, he does not perform refractive lensectomy on patients younger than 55 years old. For patients younger than 55 in Europe, he has access to the Artiplus iris-fixated lens (Ophtec), which he’s had success with.
“After the age of 55, we do refractive lensectomy, and the implant we decide on depends on the patient and the condition of the retina, but we use a lot of asymmetrical lenses and other lenses that are diffractive,” Dr. Alió said, adding that he’ll sometimes use monofocal lenses depending on the power needed and status of the macula.
For hyperopes, Dr. Alió said refractive lensectomy is an option even at younger ages in his practice due to the low risk of retinal complications and macular edema. Many lenses can be used for these patients, but his favorites are EDOF and accommodative IOLs.
Dr. Alió said that they have not had good results with the ICL and avoid it in the dysfunctional lens syndrome patient, in part due to its limited near vision gain. Dr. Alió said for younger patients, LASIK is still a good option as well.
Twenty-plus years ago, Dr. Stahl said it was frustrating trying to discuss refractive lens exchange with someone who didn’t have a cataract but couldn’t be shown diagnostically why you were recommending that procedure for them, not to mention the lens technologies were not as advanced. Fast forward to today, Dr. Stahl said it is a wonderful experience both diagnostically and surgically. “It’s such a nice conversation now because patients understand it. It’s been a fun ride through the last 20-plus years and seeing how this has evolved.”
About the physicians
Jorge Alió, MD, PhD
Professor and Chairman of Ophthalmology
University Miguel Hernández of Elche
Alicante, Spain
Jason Stahl, MD
Durrie Vision
Overland Park, Kansas
George Waring IV, MD
Waring Vision Institute
Mt. Pleasant, South Carolina
Reference
- Alió JL, et al. Crystalline lens optical dysfunction through aging. Ophthalmology. 2005;112:2022–2029.
Relevant disclosures
Alió: AkkoLens, Bausch + Lomb, Biotech, Ophtec, Zeiss
Stahl: None
Waring: None
Contact
Alió: jlalio@vissum.com
Stahl: jstahl@durrievision.com
Waring: gwaring@waringvision.com