Cornea
April 2022
by Ellen Stodola
Editorial Co-Director
While it’s hard to determine the incidence of meibomian gland dysfunction (MGD) in children, it can be a serious issue in this population. Preeya K. Gupta, MD, and Gerami Seitzman, MD, discussed MGD in pediatric patients and what to look for.
Dr. Seitzman said that the incidence of MGD in children is not well described. Clogged meibomian glands can be a cause of dry eye in children, and they can also cause bumps in the eyelids (styes or chalazia).
Dr. Seitzman noted that MGD can often be overlooked in the younger patient population because many children are not examined at the slit lamp, which is required to assess meibomian health. Also, chronic recurrent red eyes can be incorrectly attributed to “just pink eye” in this school-age population, she added.

Dr. Gupta also said that it’s hard to find published data and prevalence of MGD in children, but MGD in this population definitely exists. “What we’re noticing clinically is that patients are presenting younger and younger to us,” she said. Those in their late teens presenting with MGD may or may not be symptomatic, but over time, they do become symptomatic. “The prevalence is likely higher than we recognize,” she said.
Dr. Gupta added that part of the problem, and perhaps why these patients are not being diagnosed as often, is because “at the age of the population, we rely on them to have some sort of symptoms.” Since these patients are not necessarily coming in for routine vision screening, it may be hard to catch. “We do know that MGD can often be asymptomatic in its early phases, so that might contribute to some of the lack of information out there,” she said.
In terms of diagnosis, Dr. Gupta said that clinicians can see MGD by looking at the meibomian glands and the quality of oil coming out of the glands. “But we can also be screening patients by assessing for symptoms,” she said. “Sometimes they don’t attribute symptoms they’re having to a diagnosis like MGD.” These can include fluctuating vision, eye fatigue, or irritation.
Rosacea can happen when facial sebaceous glands become inflamed, Dr. Seitzman said. “Meibomian glands on the lids are sebaceous glands; when they are inflamed patients can be diagnosed with ocular rosacea,” she said.
The pediatric population can also be afflicted with ocular rosacea. Rosacea is commonly thought of in patients with pale skin as the inflammatory changes on their skin appear quite red. However, rosacea can happen in patients with any skin color. “Rosacea and ocular rosacea can be misdiagnosed or diagnosed late in children with skin of color, as the blood vessel changes can be more subtle with less contrast,” she said.
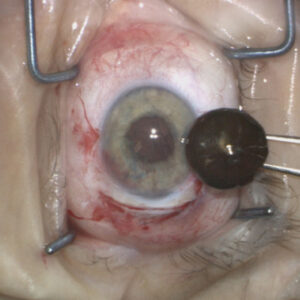
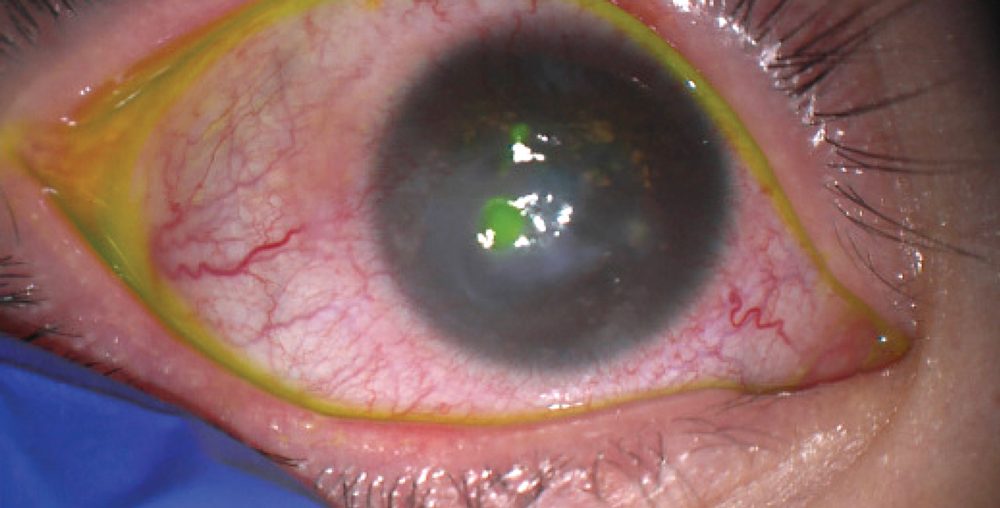
In the pediatric population, Dr. Seitzman said that styes alone or mild dry eye will be uncomfortable but reasonably easy to treat. “However, there is a markedly inflammatory condition of MGD in the pediatric population, similar to ocular rosacea,” she said. “This is called chronic blepharokeratoconjunctivitis (BKC) of childhood. Here the lid margin inflammation spills over to the surface of the eye, and the cornea can become inflamed and even infected.” When corneal involvement occurs, this is typically very painful and places children at risk of vision loss.
Dr. Seitzman said that any child with chronic recurrent red eyes, especially with photophobia and/or vision loss, should be evaluated by an ophthalmologist familiar with diagnosis and management of MGD in children and BKC in general.
MGD has the potential to be a long-term issue for these patients. If it’s not diagnosed and addressed in the early stages, many years of inflammation can cause damage to the glands and eventually meibomian gland atrophy, Dr. Gupta said. Once you get to the point of atrophy or actual loss of meibomian gland tissue, the glands can’t be restored.
Source (all): Gerami Seitzman, MD
Dr. Gupta stressed the importance of meibography or meibomian gland imaging, which will indicate what the health of the glands are and whether there has been gland loss. “Sometimes we’re surprised by how much atrophy is present on meibography, and that can give us clues as to how significant the disease is,” she said.
Once gland atrophy has set in, there isn’t currently a way to restore or repopulate those glands, Dr. Gupta said. Those patients become significantly harder to treat because they have a higher disease severity.
In terms of treatment options, Dr. Gupta suggested lid hygiene and warm compresses. “Those are things that can be done in a pediatric population,” she said, adding “you’re at the mercy of the child’s ability to comply with therapy.”
For patients who have recurrent bouts of blepharitis and inflammation, Dr. Gupta suggested oral azithromycin.
Eye drops containing antibiotic and/or steroids are often required for some length of time to help bring the disease process under control, Dr. Seitzman said. Treatment requires close follow-up to monitor the effect and for complications.
For older children who can comply with in-office MGD therapies, Dr. Gupta suggested LipiFlow (Johnson & Johnson Vision), thermal pulsation, TearCare (Sight Sciences), and iLux (Alcon). She noted that these treatments are technically off label but said she has used them for patients in the 12–14 age range because they can be compliant and are accepting of the treatment.
Dr. Gupta has done several studies in the pediatric population. One study looking at children ages 4–17 found 41% of the participants had meibomian gland atrophy.1 “This tells us that meibomian gland atrophy is present in the pediatric population, and patients with the greater atrophy are at greater risk for becoming symptomatic in the future,” she said.
She has also looked at how nutritional status and BMI may affect the pediatric population.2 This study found that patients with higher BMI had more gland tortuosity. “Instead of vertical architecture, they were sideways,” she said, which may be a precursor for atrophy.
Dr. Seitzman and colleagues Julie Schallhorn, MD, and Julius Oatts, MD, have initiated an international consortium at the University of California San Francisco called the pediatric corneal disease consortium (PCDC).
“Our first mission is to objectively study the incidence, present treatment patterns and historical visual outcomes of children with BKC,” Dr. Seitzman said. “Our goal is to use the information to inform a prospective clinical trial to help this population.”
About the physicians
Preeya K. Gupta, MD
Triangle Eye Consultants
Durham, North Carolina
Gerami Seitzman, MD
Medical Director
Francis I. Proctor Foundation for Research in Ophthalmology
University of California, San Francisco
San Francisco, California
References
- Gupta PK, et al. Prevalence of meibomian gland atrophy in a pediatric population. Cornea. 2018;37:426–430.
- Gupta PK, et al. Association of meibomian gland architecture and body mass index in a pediatric population. Ocul Surf. 2020;18:657–662.
Relevant disclosures
Gupta: Alcon, Johnson & Johnson Vision, Sight Sciences
Seitzman: None
Contact
Gupta: pgupta@TriangleEyeNC.com
Seitzman: Gerami.Seitzman@ucsf.edu