Cornea
April 2022
by Ellen Stodola
Editorial Co-Director
Rosacea can be a significant problem for many patients and may be more prevalent than physicians think. Depending on the subtype, there may be ocular involvement. Albert Cheung, MD, Vincent de Luise, MD, and Henry Perry, MD, discussed treatment strategies, in addition to sharing what to look for and how to diagnose.

Signs of oculocutaneous rosacea and diagnosis
Dr. Perry said rosacea is a chronic disease that usually starts when patients are in their 20s or 30s. It’s a disease that has a fairly high prevalence, up to 10% in some parts of the country. He added that diagnosis is mainly one of inspection by people who have treated the disease for a long time or have it themselves. Many patients have the disease and aren’t aware of it.
There are four types of rosacea, but usually we think of it being vascular or inflammatory, Dr. Perry said.
For ophthalmologists, the most important part of rosacea is ocular rosacea, Dr. Perry said, but the other three are important as well because 50% of patients in those groups also have ocular symptoms. These include erythematotelangiectatic rosacea, papulopustular rosacea, and phymatous rosacea.
Erythematotelangiectatic rosacea is a common form where there is scaling of the skin usually in the central face. Patients may have a tendency to flush, which can be exacerbated by cold, heat, alcohol, or sunlight. Papulopustular rosacea usually occurs in the central face and may look like acne vulgaris. Phymatous rosacea is commonly identified by a large bulbous nose and is caused by proliferation of vessels, hypertrophy of sebaceous glands, and thickening skin.
Dr. Cheung said that cutaneous signs include erythema/flushing, papules and pustules, telangiectasias, and rhinophyma. While ocular symptoms are often related to burning, itching, redness, and foreign body sensation, the most common signs are meibomian gland dysfunction and blepharitis. “These patients can also have conjunctival injection, phlyctenules, and keratitis, ranging from superficial punctate keratitis to marginal infiltrates and ulceration.”
In order to diagnose, Dr. Cheung said it helps to take a step back and look at facial features. Close examination of the eyelids at the slit lamp is also important, noting the presence of telangiectasias and hyperemia, presence of meibomian gland expression with pressure, quality of meibum, and presence of inspissation. Dr. Cheung added that there may be chalazia/hordeola or history of these. Fluorescein can help highlight the previously mentioned corneal findings and lissamine green the conjunctival changes.
This issue is more common in women and among patients middle-aged or older, Dr. Cheung said.
Rosacea can flare up in response to certain triggers such as sun exposure or emotional stress, Dr. de Luise said.
He said that a newer, updated classification of rosacea by the American Academy of Dermatology is now by phenotype. “Using a targeted therapy for each of these phenotypes/subtypes is now the preferred strategy of care by dermatologists,” he said.1
Impact of oculocutaneous rosacea on the ocular surface
Dr. de Luise discussed the corneal and ocular surface manifestations of ocular rosacea, which he described as protean and including anterior blepharitis, posterior blepharitis (meibomitis and meibomian gland dysfunction), eyelid telangiectasias, madarosis, punctate epithelial keratopathy, chalazion formation, corneal neovascularization, subepithelial infiltrates, and spade-like peripheral infiltrates.
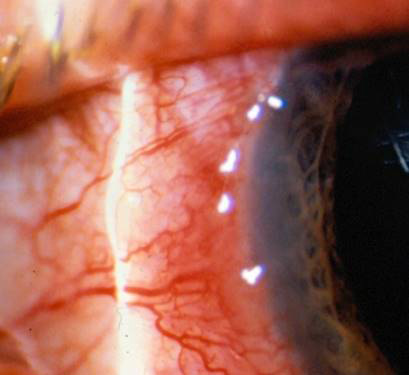
Source (all): Vincent de Luise, MD
Some of the dermatological aspects of rosacea, such as facial flushing, are reversible. Other changes, such as severe rhinophymatous nasal changes, may be long lasting, he said.
Oculocutaneous rosacea can lead to inflammation with associated ulceration and scarring, Dr. Cheung said. Superficial changes can often be improved or reversed. “In the later stages, it can be difficult to reverse stromal thinning, scarring, or the associated neovascularization that develops,” he said.
Dr. Perry said that ocular rosacea needs to be treated months before cataract surgery. He added that Demodex folliculorum is frequently associated with rosacea, noting the importance of treating the Demodex infestation before surgery as well. “You have to look at the eyelashes and see if there is cylindrical dandruff,” he said. The cylindrical dandruff indicates in 80–90% of patients the presence of Demodex mites. Patients may also have ocular inflammation. “You have to think of treating not only the rosacea because that will reflect the presence of increased amounts of bacteria, but you have to also eradicate the Demodex,” Dr. Perry said. Demodex carry Staph bacteria on their surface and Bacillus oleronius and cereus in their gut.
Treatment strategies
Patients with oculocutaneous rosacea benefit from avoiding triggers, such as certain foods, beverages, medications, and environments that exacerbate flushing, Dr. Cheung said. Additionally, certain systemic antibiotics (e.g., oral doxycycline/tetracycline, azithromycin) can treat both ocular and cutaneous rosacea. Other treatment strategies are based on the type of ocular pathology, he said.
Meibomian gland dysfunction and blepharitis treatment often begins with conservative treatments. “This can include warm compresses, eyelid scrubs, and digital massage,” Dr. Cheung said. “Other therapies include oral omega-3 fatty acid supplementation, topical antibiotics, microblepharoexfoliation, heat application with/without eyelid mechanical stimulation, meibomian gland probing, and intense pulsed light.”
Related dry eye can benefit from frequent preservative-free artificial tears/ointments, punctal occlusion, anti-inflammatory agents (cyclosporine, lifitegrast, low-dose topical corticosteroids), and autologous serum tears, Dr. Cheung said. Treatment of conjunctivitis and keratitis may benefit from topical corticosteroids and anti-inflammatory agents. If there is any infiltrate or ulceration, cultures and topical anti-microbial treatment is advised prior to corticosteroids, he said.
“For severe ocular surface disease, scarring and thinning may cause irregular astigmatism and benefit from a hard contact lens for visual rehabilitation,” Dr. Cheung said. “Although rare, stromal thinning and perforations may need a bandage contact lens, cyanoacrylate gluing, amniotic membrane, tarsorrhaphy, conjunctival flap, and/or lamellar keratoplasty.”
Dr. Cheung noted that he does not have much experience with meibomian gland probing and intense pulsed light, but he has found the other treatment options effective with a patient-specific regimen.
Dr. Perry noted that there are several good treatments for rosacea. However, he said that one problem is that a lot of clinicians don’t realize that sometimes steroids may make acne rosacea worse.
For ocular rosacea, steroids and doxycycline systemically have good results, he said, but if the patient has another form of rosacea, which is not uncommon, steroids are a double-edged sword. “I like to limit steroids to patients who just have the ocular form of rosacea,” he said. Dr. Perry added that ivermectin and metronidazole are effective treatments. You can combine this with the tetracycline family of antibiotics, including doxycycline and minocycline and minimize corticosteroid use.
Dr. Perry said he has been using BlephEx and microblepharoexfoliation for the last 5 years with good results. He added that many use tea tree oil and Cliradex (Bio-Tissue) as well.
There is some evidence that diets high in omega-3 essential fatty acids may be beneficial in rosacea, Dr. de Luise said, adding that there are several oral and topical options for rosacea, with variable degrees of efficacy. Dr. de Luise noted a number of other treatment options (see sidebar).
Dr. de Luise also mentioned the “interesting relationship” between Demodex mite infiltration of the eyelid margin. “Studies have been done to determine if this is correlative or causative,” he said. “To that end, Tarsus Pharmaceuticals is developing TP-03 (lotilaner), a mite-specific GABA antagonist, for topical use on the eyelids and facial skin as a treatment for anterior blepharitis due to Demodex and is also testing a TP-04 formulation as a treatment for rosacea.”
He said that AiViva BioPharma is testing an intradermal delivery of its pipeline molecule AIV001 in subjects with papulopustular rosacea. CAGE Bio is testing its pipeline gel CGB-400 for inflammatory rosacea. Allergan is developing AGN-199201 oxymetazoline cream for topical use and evaluating utility in subjects with
erythema and rosacea.
Contraindications
In terms of contraindications, Dr. de Luise said that topical ophthalmic corticosteroids should be used with great caution in the management of rosacea. “It turns out that rosacea keratitis is extremely sensitive to topical corticosteroids, and corneal ulceration, descemetocele formation, and perforation have been reported to occur,” he said. “If topical corticosteroids are to be used in the management of rosacea keratitis, an ester steroid such as loteprednol etabonate is preferred, and careful, close follow-up is strongly recommended.”
Dr. Cheung noted that certain oral antibiotics may have tolerability issues. Topical corticosteroid use needs to be monitored as certain eyes may be susceptible to corneal melts, he added. “I would avoid corticosteroids if infectious keratitis is suspected until properly treated.”
Dr. Cheung said he cautiously uses topical corticosteroids for acute conjunctival/corneal disease to help quiet the eye. For dryness and chronic aspects of the disease, corticosteroids may be used initially as bridge therapy while nonsteroidal anti-inflammatories such as cyclosporine or lifitegrast are taking their effect.
Article sidebar
Dr. de Luise shared details on several treatment options for rosacea:
- Oral minocycline or oral doxycycline: This is a commonly employed strategy, especially in a modified release 40-mg formulation of doxycycline. These various oral cyclines should not be used for longer than 3–4 months at a time followed by a hiatus. Side effects of the cyclines are well known and include gastroenteritis, vaginal candidiasis, and dermal skin rashes.
- Topical ivermectin 1% cream: This is used with fairly good success in several of the subtypes of rosacea. It directly targets Demodex folliculorum and Demodex brevis.
- Topical brimonidine in a 0.33% gel: This targets vasomotor dysregulation in rosacea. Topical brimonidine is sometimes used in concert with topical potassium titanyl phosphate to address persistent facial erythema in rosacea.
- Topical oxymetazoline: This is an imidazole whose mechanism of action is as an alpha 1A and alpha 2A adrenoreceptor agonist that induces vasoconstriction of dilated vessels in rosacea.
- Topical isotretinoin: This has some degree of efficacy.
- Another imidazole, metronidazole: These have been used in a topical formulation in facial rosacea. An ophthalmic formulation has been tested but is not available.
- Intense pulsed light therapy: This has had some degree of success in rosacea.
About the physicians
Albert Cheung, MD
Virginia Eye Consultants
Norfolk, Virginia
Vincent de Luise, MD
Assistant Clinical Professor of Ophthalmology
Yale University School of Medicine
New Haven, Connecticut
Henry Perry, MD
Chief of the Cornea Service
NuHealth Medical Center
East Meadow, New York
Reference
- Gallo RL, et al. Standard classification and pathophysiology of rosacea: The 2017 update by the National Rosacea Society Expert Committee. J Am Acad Dermatol. 2018;78:148–155.
Relevant disclosures
Cheung: None
De Luise: None
Perry: Alcon, Allergan, Azura, AXIM, Bausch + Lomb, BlephEx, NovaBay, Novaliq, Noveome, Omeros, Sol-Gel, Tarsus
Contact
Cheung: ACheung@cvphealth.com
De Luise: vdeluisemd@gmail.com
Perry: hankcornea@gmail.com


