ONLINE EXCLUSIVE
Cataract
Summer 2026
by Ellen Stodola
Editorial Co-Director
In an article published in the JCRS Online Case Reports,1 Andreas F. Borkenstein, MD, and colleagues discussed the “No ring approach technique for Nd:YAG capsulotomy in pinhole intraocular lenses: mask-sparing strategy to prevent occluder ring damage.” Dr. Borkenstein spoke with EyeWorld to share highlights from the report, why the technique is important, and when it applies.
Dr. Borkenstein noted that he collaborated with Liliana Werner, MD, PhD, who has long-time expertise in IOL pathology, and Kevin M. Miller, MD, who brings extensive clinical and surgical experience. Their perspectives helped to strengthen both the scientific foundation and the practical relevance of this work, he said.
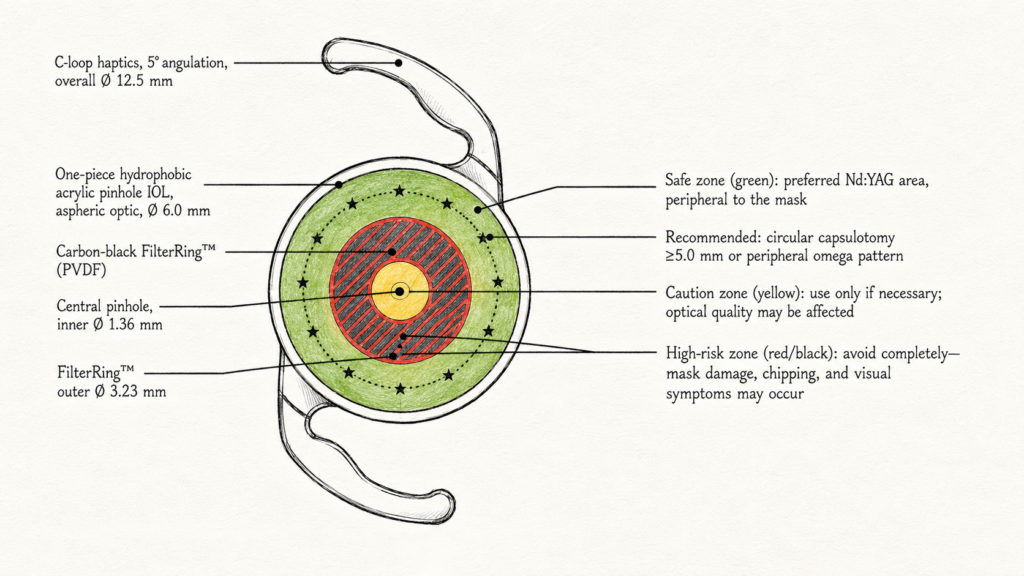
Source: Andreas F. Borkenstein, MD
According to Dr. Borkenstein, the development of the no ring approach (NORA) was a direct consequence of earlier experimental work, where he and colleagues investigated the effects of Nd:YAG laser energy on different intraocular lens materials.2
“We observed that while conventional hydrophobic acrylic optics typically show only minor pitting, the response of the carbon-black, opaque mask used in small-aperture IOLs was fundamentally different—laser hits led to extensive structural damage, including fragmentation and significant material loss,” he said. “What was particularly striking to us was that this level of damage could occur even with routine energy settings or a single shot.” He added that this raised an important clinical concern: A complication that might be negligible in standard IOLs could become visually significant and potentially devastating in a pinhole design.
After publishing on this, Dr. Borkenstein said that he received many communications from colleagues around the world, sharing their own clinical experiences. “Several reported real-world cases of inadvertent Nd:YAG laser application to the mask, resulting in visual disturbances such as dysphotopsia and, in some cases, the need for IOL exchange,” he said. “These reports confirmed that this was not just a theoretical or laboratory issue but a clinically relevant and likely underrecognized problem in pinhole IOLs.”
Dr. Borkenstein said that the combination of experimental evidence and clinical feedback prompted additional action. “In collaboration with [Dr.] Werner and [Dr.] Miller, I developed the NORA technique as a practical, safety-oriented strategy,” he said. “The primary goal was to translate material-specific vulnerability into a clear and reproducible clinical approach, while also raising awareness among surgeons that Nd:YAG capsulotomy in eyes with small-aperture IOLs requires a higher level of precision and caution.”
He noted that it’s hard to pinpoint the exact incidence of this issue. While the frequency of Nd:YAG capsulotomy itself is well established, the rate of inadvertent mask hits is likely underreported. “However, based on both the physical properties of the material and the clinical cases described, even a single misapplied laser shot can have disproportionate consequences,” Dr. Borkenstein said. “For that reason, we think the issue is less about how often it occurs and more about the severity of the outcome when it does. This is precisely why a preventive strategy like NORA is so important.”
Dr. Borkenstein said that patient counseling remains an important part of the process, but it should be balanced and not create unnecessary concern. Nd:YAG laser capsulotomy is a well-established and highly effective procedure that has been the gold standard for treating posterior capsule opacification for many years, he said, adding that the technology itself is very reliable, and in most cases, it is performed safely and efficiently.
“That said, when dealing with small-aperture IOLs, we do take a slightly different approach in how we communicate with patients. We briefly explain that their lens has a unique design and that this requires an even higher level of precision during the laser procedure,” he said. “The goal is not to alarm the patient but to help them understand why cooperation is particularly important in this setting.”
One key aspect is the need to remain steady and to maintain fixation throughout the procedure. “From our experience—and as is well known from other types of IOL-related laser complications—sudden eye movements or loss of fixation are among the most common reasons for unintended laser application and IOL damage,” Dr. Borkenstein said. “By setting expectations, patients tend to be more focused and compliant, which directly contributes to procedural safety.”
Dr. Borkenstein stressed that awareness should not be limited to the surgeon and patient alone. “It is equally important that the entire clinical team—technicians, assisting staff, and anyone involved in patient preparation—understands that these are not entirely routine cases. Raising this level of awareness helps ensure optimal setup, careful patient positioning, and a more controlled environment overall.”
While the fundamental principles of Nd:YAG capsulotomy remain the same, performing the procedure in eyes with small-aperture IOLs requires a more deliberate and controlled approach, Dr. Borkenstein said.
“One of the most important steps is ensuring adequate pupil dilation. Taking the time to wait until the pupil is fully dilated significantly improves visualization of the mask and the surrounding peripheral, safe zones, which is critical for precise shot placement,” he said, adding that rushing this step can unnecessarily increase the risk of misalignment.
“We also recommend working without time pressure and adopting a slower, more stepwise technique,” he said. “Each laser shot should be placed carefully, with continuous confirmation of proper focus on the posterior capsule rather than the IOL. Maintaining a posterior offset is particularly important to keep the photodisruptive effect safely behind the lens.”
Additionally, Dr. Borkenstein advised physicians to use a contact lens in every case, which can help stabilize the eye, improve focusing accuracy, and allow for better control of the laser energy.
“In addition, surgeons should consciously adopt the mask-sparing strategies described in the NORA technique—either working within the central aperture or in the peripheral clear optic—while in any case, strictly avoiding the carbon-black mask at all times,” he said. “This represents a subtle but important mental shift: Unlike routine capsulotomy, where occasional minor IOL pitting may be tolerated, in these lenses even a single hit to the mask must be avoided.” Overall, the key adaptations are increasing precision, slowing down, and maintaining constant awareness of the unique risk profile of these lenses.
In Dr. Borkenstein’s practice, the principles of the NORA technique are applied consistently when using Nd:YAG capsulotomy in eyes with small-aperture IOLs. “It has essentially become our standard approach in these cases, as it directly reflects the material-specific risks we have identified,” he said.
Beyond personal experience, he said this concept has been discussed informally with other colleagues at international meetings. “The feedback afterward has been very consistent—many surgeons recognize this as a relevant and important issue, particularly those who have either encountered similar complications or are aware of the unique vulnerability of these lenses,” he said. “This was one of the main motivations for publishing the technique: to extend awareness beyond conference discussions and reach a broader audience, including colleagues who may not regularly attend such meetings. In addition, the companies that manufacture pinhole lenses should be aware of this and should incorporate these aspects when introducing new IOLs in order to raise awareness.”
Dr. Borkenstein emphasized that the NORA technique should be understood as an evidence-informed, preventive strategy rather than a formally validated clinical protocol. “As outlined in our paper, prospective controlled studies in this area are difficult to conduct,” he said. “The complication we are trying to prevent should be relatively rare but is potentially very severe, and it would not be practical—or ethical—to study it in a controlled, randomized fashion.” Ultimately, Dr. Borkenstein thinks the rationale for the NORA technique is straightforward because of the irreversible nature of mask damage. “Even in the absence of large-scale clinical trials, a careful, preventive strategy is both justified and necessary,” he said.
About the physician
Andreas F. Borkenstein, MD
Borkenstein & Borkenstein Private Practice
Privatklinik der Kreuzschwestern
Graz, Austria
References
- Borkenstein AF, et al. No ring approach technique for Nd:YAG capsulotomy in pinhole intraocular lenses: mask-sparing strategy to prevent occluder ring damage. JCRS Open. 2026;14:e00232.
- Borkenstein AF, et al. Incorrectly focused neodymium:yttrium-aluminum-garnet (Nd:YAG) laser beam leads to massive destructive effects in small-aperture (pinhole) intraocular lenses. Ophthalmol Ther. 2024;13:2745–2758.
Relevant disclosures
Borkenstein: None
Contact
Borkenstein: crustalith@gmx.at



