Cataract
Spring 2026
by Ellen Stodola
Editorial Co-Director
Having varying degrees of zonulopathy can make a case more challenging. D. Brian Kim, MD, and Angela Verkade, MD, discussed what they look for to determine if a patient has some form of zonulopathy, the best lenses and tools to use in these cases, and other important approaches to proceeding with surgery.
Signs of zonulopathy
Dr. Kim said there are several signs he looks for to determine if a patient has some form of zonulopathy. He first noted pseudoexfoliation on the anterior lens capsule. He also indicated phacodonesis and said that he will ask the patient to move the eye side to side and up and down, looking for a wobbly lens/bag complex. “A dense cataract in one eye with a comparatively minimal cataract in the other eye may suggest trauma, which is associated with zonulopathy,” Dr. Kim said.
A shallower anterior chamber depth in one eye compared to the other eye on optical biometry suggests zonulopathy. “Hypermature cataracts, advanced age, prior ocular trauma, prior retinal surgery, prior angle closure glaucoma attack, retinitis pigmentosa, and uveitis are risk factors for zonulopathy,” Dr. Kim said. Finally, he said that family history of hereditary lens abnormalities, such as Marfan syndrome and homocystinuria, can be warning signs.
Dr. Verkade stressed the importance of the preoperative exam in preparing for cases with zonulopathy. She said that asking the patient about history, especially history of trauma or ocular trauma, is crucial, as well as taking a history of tissue disorders. Slit lamp signs, like asymmetric dilation on one side, might be suggestive of zonulopathy on that side. Pseudoexfoliation on exam, colobomas, aniridia, or asymmetric cataracts (like a hypermature cataract on one side) can be associated with zonulopathy, she said.
Phacodonesis, Dr. Verkade continued, is suggestive of severe zonulopathy, and it’s important to check these patients before dilation as it is often easier to see phacodonesis pre-dilation. Any decentration of the lens after dilation is suggestive of zonulopathy as well.
It’s also important to look for other entities that are associated in their history, such as a previous vitrectomy, high myopia, history of uveitis, or other retinal disorders.
With imaging, you might see an asymmetric anterior chamber depth on your biometry in cases of zonulopathy. You can obtain a UBM preoperatively that might be helpful to identify the location and extent of zonulopathy, she said.
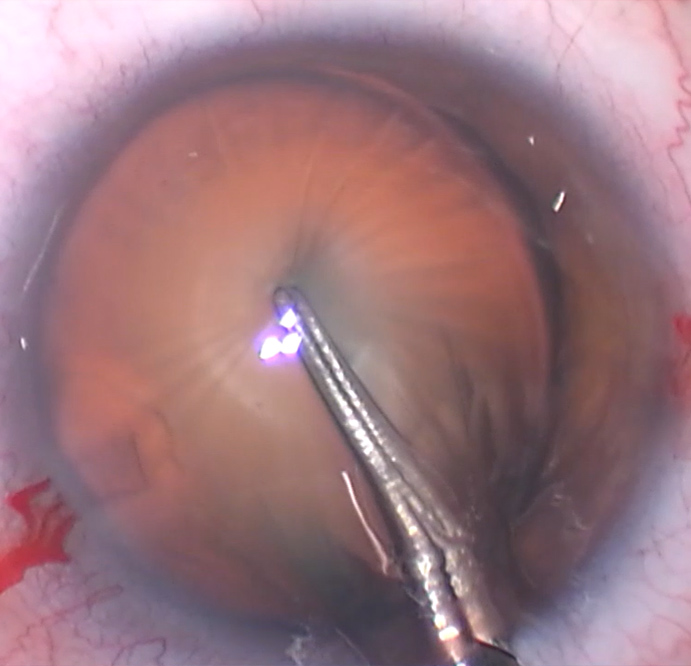
Source: D. Brian Kim, MD
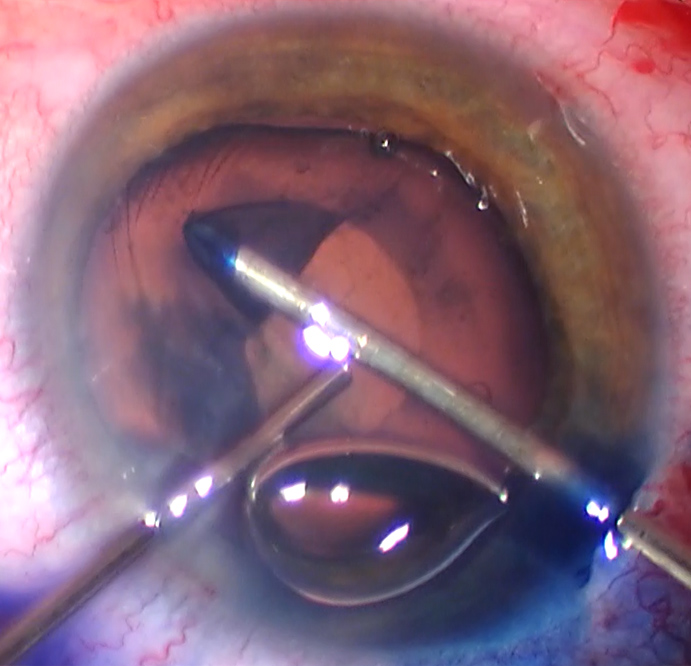
Source: D. Brian Kim, MD
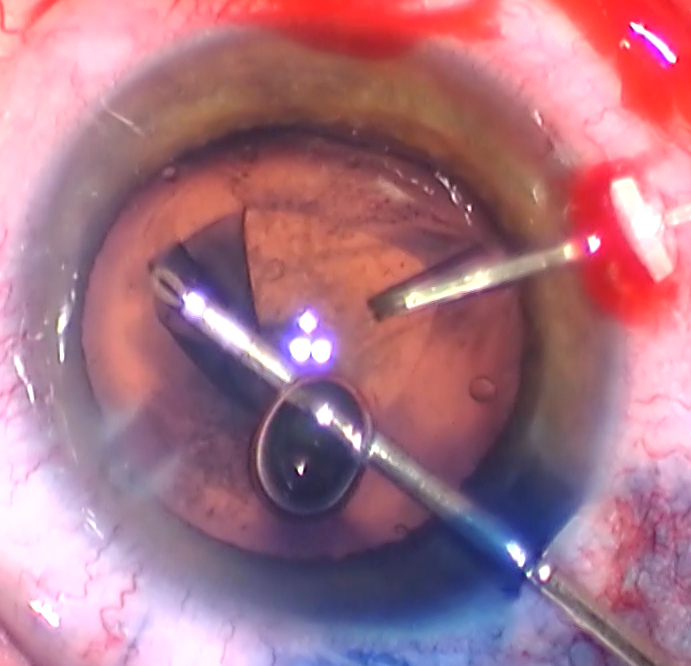
Source: D. Brian Kim, MD
Lenses for mild zonulopathy
When choosing a lens, Dr. Kim said a three-piece acrylic IOL is preferable to a single-piece acrylic IOL. “In my opinion, a three-piece IOL provides more equatorial capsule support due to the relative stiffness of the haptics,” he said. “Furthermore, if the IOL/bag complex subluxates in the future, one can scleral fixate the existing three-piece IOL, which for me is the Sensar AR40 lens [Johnson & Johnson Vision], to perform the Yamane technique.”
Although studies have shown that a CTR does not prevent lens/bag dislocation, a CTR is helpful if the lens/bag complex dislocates in the future by scleral suture fixating the lens/bag/CTR complex, Dr. Kim said. Sulcus fixation with optic capture with a three-piece IOL is another strategy that can be used to minimize capsule contraction, which can stress the zonules. “In my opinion, this is a good option for mild zonulopathy but not for severe cases.”
Dr. Kim said he encounters mild zonulopathy regularly, and it occurs with hypermature cataracts, post-vitrectomized eyes, post-trauma, and pseudoexfoliation.
Dr. Verkade said her preference is a three-piece IOL. If you have a case of mild or diffuse zonulopathy, a three-piece IOL, particularly coupled with a CTR, can make the bag complex much more stable. Additionally, Dr. Verkade said that placing a three-piece IOL or a CTR allows her to have something to fixate later in case there is further dislocation down the road.
Zonulopathy during surgery
Dr. Kim said there are also signs of zonulopathy while doing a case. “A keen awareness and active observation are required so that you are not taken off guard to avoid iatrogenic zonular dehiscence or posterior capsule rupture.”
Starting from the beginning of the case, he mentioned several signs to look out for:
- Filling the anterior chamber with OVD: The lens/bag complex may push backward much more than it should, he said.
- Puncturing the anterior capsule: Dr. Kim said the spider sign is when you attempt to puncture the central anterior capsule, but it fails to puncture and simply pushes backward from lack of zonular support, resulting in striae that looks like a spider. “A sharp instrument or two-handed technique may be required to grasp and fixate the capsule with forceps while puncturing with the other hand with a cystotome or sharp forceps.”
- Striae folds within the capsulorhexis flap: The lack of zonular support causes striae and difficulty pulling the rhexis flap with hypermobility of the lens/bag complex. Dr. Kim said adding capsule retractors is helpful for counter fixation.
- Hyper-deepening of the AC from infusion pressure: When placing the phaco probe in the eye, the infusion pressure can cause an unusually deep AC from the lens/bag complex being pushed backward. “If there is reverse pupillary block, you can lift the pupillary edge to break it,” Dr. Kim said. Consider switching to a lower flow setting, i.e., lower the bottle height, lower vacuum, and be judicious with ultrasound. However, lower infusion pressure means the chamber might be less stable, and careful foot pedal modulation is necessary to avoid chamber shallowing.
- Difficulty spinning the lens after hydrodissection: Trouble spinning the lens despite achieving a successful wave is a sign that the lens-to-bag adhesions are stronger than the zonules. “You should avoid trying to spin the lens with brute force, which will only rip more zonules, and instead employ a no-rotation lens disassembly technique,” Dr. Kim said.
- Less effective sculpting: If you notice that the lens doesn’t cut well while sculpting, this can be from lack of zonular support, which causes the lens to push backward with each sculpt maneuver. “Try increasing the phaco setting for more effective sculpting,” he said. “Alternatively, you can place a chopper around the contralateral lens equator to hook and support the lens as you push down to sculpt.”
- Difficulty pulling lens pieces out of the bag: Pulling pieces out of the bag requires you to first embed then impale the phaco tip into the lens material, which is more difficult when there is zonulopathy, Dr. Kim said. Since the bag is floppier, it may be more adherent to the lens pieces and may collapse into the phaco tip when applying vacuum, which increases the risk for posterior capsule rupture. “Use a second instrument such as the chopper to get around the lens piece from the capsule fornix, and pull it out of the bag from behind,” he said. “Alternatively, you can try and re-hydrodissect or viscodissect the lens off the adherent capsular bag. This is a more gentle, effective, and safer strategy.”
- Difficult cortical removal: “You have to be very careful with high aspiration and vacuum because you can inadvertently grab the capsular bag and rip more zonules,” Dr. Kim said. “If you grab the bag, stop and initiate reflux to release the capsule material.” He added that careful foot pedal control with lower levels of aspiration and vacuum are essential to prevent ripping more zonules. A low flow polish setting is helpful to gently remove the fine lens material. “Alternatively, you can use an irrigating cannula used for polishing. If the material is too difficult to remove, it’s best to leave it and place the IOL,” he said. “You can always perform a YAG capsulotomy later if needed.”
It’s important to have a diverse toolbox when it comes to these cases, Dr. Verkade said, because not every zonulopathy case is going to behave the same. Depending on the case and the severity of zonulopathy, she said she may use different techniques.
“I usually like to start out with combining the use of a dispersive viscoelastic and filling the remainder of the anterior chamber with a high molecular weight cohesive viscoelastic. Using the dispersive viscoelastic becomes even more important, especially if you have a hypermature cataract or a white cataract coupled with zonulopathy and you need to use trypan to stain your capsule,” she said. In these cases, Dr. Verkade prefers to use the dispersive viscoelastic to tamponade the areas of zonulopathy and stain the anterior capsule with a trypan using the “paint technique,” where you paint it underneath the viscoelastic. This allows you to avoid filling the whole anterior chamber with trypan blue and risk trypan entering through the area of the zonular loss. This will cause the red reflex to turn blue, making the case more challenging.
“During the rhexis if you’re seeing signs of wrinkling of the capsular bag, I like to grab a second instrument in my non-dominant hand,” she said, which allows her to have countertraction on the capsular bag opening. Often in severe zonulopathy, there’s no tension to pull against when you’re trying to bring the flap around. “I use gentle counter-tension with a second instrument, like a Kuglen manipulator, which can often be helpful to facilitate the capsulorhexis and keep it round and centered,” she said. “I usually like to place capsular hooks as early as I can to allow for even support of the capsular bag.”
Other things she’s conscious of during the case include not overly rotating the lens when hydrodissecting. When you’re removing cortical material, remove cortex more circumferentially toward the area of zonular loss rather than pulling in centrally and radially, which can potentially make the zonulopathy worse, Dr. Verkade said. These are cases where she likes to use viscodissection as well, which can help loosen cortex and nuclear pieces and bring them up and out when needed.
For stability, when you’re inserting the lens, if there’s a mild, diffuse zonulopathy or a focal area, Dr. Verkade likes 3 to 4 clock hours or less. “Then I’ll use a CTR combined with the three-piece IOL.”
If there’s more severe zonulopathy or an area that’s more than 4 clock hours, Dr. Verkade will use a CTR with capsular tension segments in the areas of most severe zonulopathy and combine that with the three-piece IOL.
“I like to use a manual insertion technique for my CTRs, where I’ll place it through an incision that will allow for the placement of the ring toward the areas of zonulopathy, then I’ll usually have a Sinskey hook or another instrument in my second hand to allow for countertraction against the CTR to avoid pressure on the capsule and potential worsening of zonulopathy,” she said. “It allows me to get a better feel in case I run into resistance, then I can easily maneuver out and go in a different direction or through a different incision, compared to potentially using an injector for CTRs.”
Dr. Verkade likes to suture the CTR using a CV-8 Gore-Tex suture rather than prolene and use either a Hoffman pocket or bury the knots within the sclera coupled with a scleral groove. There are also capsular tension devices, like the Cionni ring, which Dr. Verkade said has a nice additional eyelet for fixation where you can put that along the area of most severe zonulopathy. If there is very severe zonulopathy or greater than 9 clock hours, Dr. Verkade opts for a secondary fixation of a three-piece IOL like the Sensar AR40. “I prefer the Yamane technique in these cases, as it requires a smaller incision compared to other techniques, and in my hands, it’s a little more efficient,” she said, though she noted that there are other techniques like a glued or sutured IOL or even anterior chamber IOL that can be used.
When dealing with more severe zonulopathy, this can make the case trickier, and Dr. Kim said, “many factors will affect your plan of attack.” He also suggested first painting the anterior capsule surface with trypan blue because this will aid with capsulorhexis, lens disassembly, and improve visualization for capsule retractor, CTR, and CTS placement. “If you are unable to perform capsulorhexis, capsule retractors are very helpful,” he said. “You want to place the retractor just behind your rhexis flap to provide counterforce.”
Dr. Kim also mentioned that using a CTR provides circumferential support. “There is debate as to when the CTR should be placed,” he said. It’s Dr. Kim’s opinion that there is no value in placing the CTR early, as this can make cortical removal more difficult. “I always place the CTR after all the lens material is removed, and I employ cross chopping techniques to bypass the need to rotate the lens,” he said. “I use a CTR injection technique to minimize torsional stress on the zonules. As the CTR is advanced, a Lester hook is placed through the leading eyelet to apply a compression force to shrink the diameter of the CTR as it is being delivered.”
Dr. Kim said that if there are more than 4 clock hours of zonular dehiscence, a CTR may not provide enough equatorial support, and therefore, scleral suture fixation with a CTS or modified CTR with eyelet can be used. “The AssiAnchor [Hanita Lenses] is another device, but it’s not available in the U.S.,” he said. “A modified CTR can be used but needs to be rotated such that the eyelet is positioned over the area of weakness which can further stress the zonules. I prefer a scleral sutured Gore-Tex CTS because I can strategically place it over the areas of zonular weakness.”
Take-home messages
Zonulopathy is not that common, Dr. Verkade said, but it is more common if you’re seeing patients post-trauma or with certain ocular diseases. We hope to catch zonulopathy preoperatively, she said, but many times, patients can have zonulopathy for unknown reasons and without obvious preoperative signs. It’s important to have a variety of tools and techniques at your fingertips. “Preparation is key, and the more we can plan and anticipate the needs preoperatively, the better the case will go intraoperatively. It’s very important to take time to practice these techniques either in a wet lab or in your OR. It’s also important to learn from experts at meetings when you can,” Dr. Verkade said.
She added that if you don’t have a chance to practice the techniques or aren’t comfortable executing them, it’s OK to leave a patient aphakic and come back, to fixate later or send to someone more comfortable with fixation if you do not routinely perform these surgeries.
Dr. Kim said the most important take-home message is to recognize this early and to avoid doing anything to worsen the zonulopathy. “You can turn a routine case into a complicated one if you don’t pay careful attention with every step of the case,” he said. “Finally, despite your best efforts, the lens-bag complex may not be salvageable, and you should have the skills to place an IOL in the absence of capsule support.”
About the physicians
D. Brian Kim, MD
Professional Eye Associates
Dalton, Georgia
Angela Verkade, MD
Clinical Assistant Professor of Ophthalmology and Visual Sciences
Kellogg Eye Center
University of Michigan
Ann Arbor, Michigan
Relevant disclosures
Kim: None
Verkade: None
Contact
Kim: kim@professionaleye.com
Verkade: ajverkad@med.umich.edu

