Cornea
Winter 2025
by Ellen Stodola
Editorial Co-Director
Ophthalmologists, particularly corneal specialists, may encounter a variety of pathogens that can cause infectious keratitis. Gerami Seitzman, MD, and Sonal Tuli, MD, MEd, MBA, went into detail on some of these infections, including those that may be considered “atypical,” and how to identify and diagnose them.
Dr. Seitzman started the discussion by acknowledging “what is odd for you may be normal for me,” particularly noting that what is “atypical” varies in different practices and patient populations around the country and around the world.
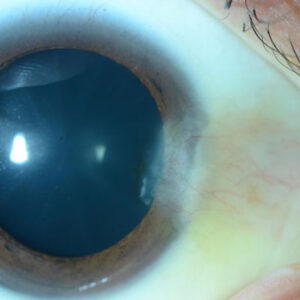
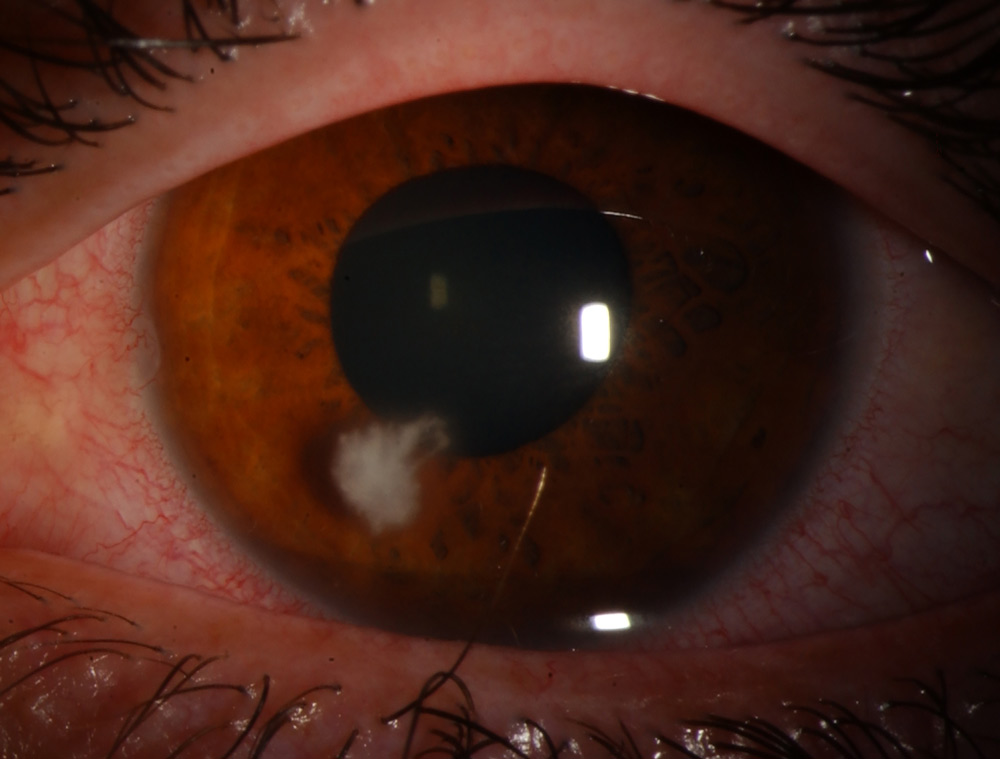
Source: Sonal Tuli, MD, MEd, MBA
An “atypical” corneal infection refers to one caused by organisms that are not commonly encountered in day-to-day practice, she said. “But what counts as atypical depends on where you are seeing patients. For example, fungal keratitis is the leading cause of infectious keratitis in South India, but in my practice in San Francisco, it’s less common cause. Similarly, Nocardia (a type of bacteria) would be considered atypical in North America or Europe, but in parts of India and South Asia, it is a more well-recognized etiology of infectious keratitis.”
For this reason, she said it’s important for ophthalmologists to define what is typical for their practice settings, their latitude, and their patient populations. “The best way to know this is to culture routinely and keep track of local surveillance data,” she said.
Dr. Seitzman said that organisms most cornea specialists would consider “typical” are bacterial pathogens, including Staphylococcus aureus, Staphylococcus epidermidis, Streptococcus pneumoniae, Pseudomonas aeruginosa, and Moraxella. “However, a common pathogen with an uncommon resistance pattern, for example a pan-resistant pseudomonas, could be considered atypical in some settings because it is unexpected,” she said. Viral keratitis from HSV or VZV is also common.
By contrast, she said that CMV, EBV, measles, and mpox are atypical viruses for keratitis. “As a general rule, organisms most cornea specialists would consider atypical include Acanthamoeba, atypical mycobacteria, Achromobacter spp., Citrobacter spp., and Pythium insidiosum.”
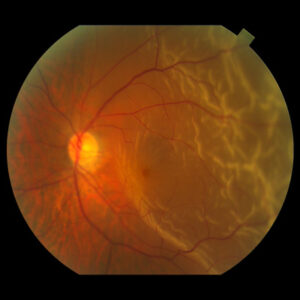
Source: Sonal Tuli, MD, MEd, MBA
A common clue for atypical keratitis is progression despite appropriate therapy for a typical infection, Dr. Seitzman said. Acanthamoeba often begins as a patchy, rough epitheliopathy, while Nocardia may present with more fine, wreath-like infiltrates. Atypical mycobacteria may present late after surgery, with indolent infiltrates at incision sites or under LASIK flaps. Pythium can mimic fungal keratitis, often with linear, tentacle-like infiltrates. Viral atypical keratitis, such as CMV endotheliitis, may show coin-shaped keratic precipitates. Recognizing these clinical patterns can sometimes raise suspicion early, Dr. Seitzman said.
Dr. Tuli agreed that the typical infectious keratitis that occurs in the U.S. is bacterial. However, she noted the fungal infections are more common in Florida and other southern states. These are atypical because they don’t respond to regular antibacterial (need antifungals), can continue to grow deeper in the cornea, and penetrate the Descemet’s membrane, even with treatment, Dr. Tuli said. Steroids are absolutely contraindicated in these cases, she said, unlike bacterial where the Steroids for Corneal Ulcers Trial (SCUT) indicated that more severe bacterial infections may benefit from early steroid therapy in addition to appropriate antibiotics.
Another atypical type of infectious keratitis that Dr. Tuli mentioned was Acanthamoeba, which she said usually occurs in contact lens wearers exposed to water sources, though it might also be seen rarely after trauma with dirt or soil. This can be slow growing and is often misdiagnosed as herpes initially. There are also no commercial medications available in the U.S. to treat this, and Dr. Tuli said treatment is often required for months.

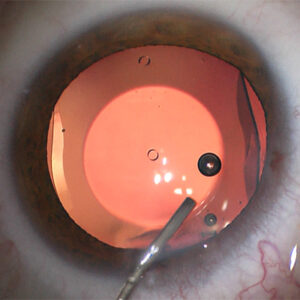
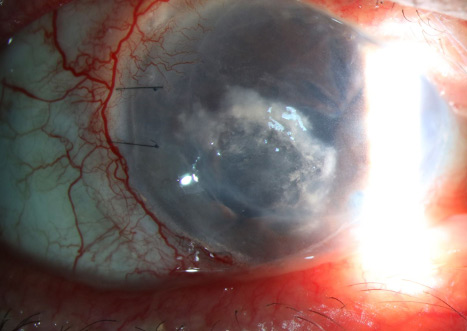
Source: Francis I. Proctor Foundation
Dr. Tuli called microsporidia an “opportunistic infection,” which was previously thought to only affect immunocompromised people. She added that it’s fairly rare in the U.S., and there is no good treatment. You can get it from swimming in untreated water, and while the epithelial disease resolves on its own or can be treated with antibiotics, like moxifloxacin or antiparasitic medications, the deeper stromal disease usually occurs in immunocompetent people, has no medical treatment, and needs a transplant to treat.
For symptoms of one of these infections, Dr. Tuli cautioned to look out for too little pain with HSV or too much pain with Acanthamoeba.
For fungus, she noted examination signs such as feathery borders, endoplaques, satellite lesions, pigmentation, or immune rings can be clues to the diagnosis. With Acanthamoeba, Dr. Tuli said to look for perineuritis or ring ulcer. With microsporidia, look for coarse, granular, popcorn-like opacities.
There are several tools that ophthalmologists can employ to help diagnose these issues for patients. A confocal microscope helps with fungal and Acanthamoeba, Dr. Tuli said. PCR testing of corneal swabs, using a commercial service such as HealthTrackRx, is another good tool for many of these infections. Culture is also an option for some of them, but she added that special stains are required in the lab for all the atypical ones, so you need to let the lab know what you are looking for. Rarely, corneal biopsy may be needed for deeper infections.
Dr. Seitzman stressed that a heightened suspicion is the first diagnostic tool. “Cultures and smears remain the standard of care, but atypical organisms are often fastidious and may require special media,” she said. Corneal biopsy, suture pass techniques, or lifting a LASIK flap may be necessary in some cases.
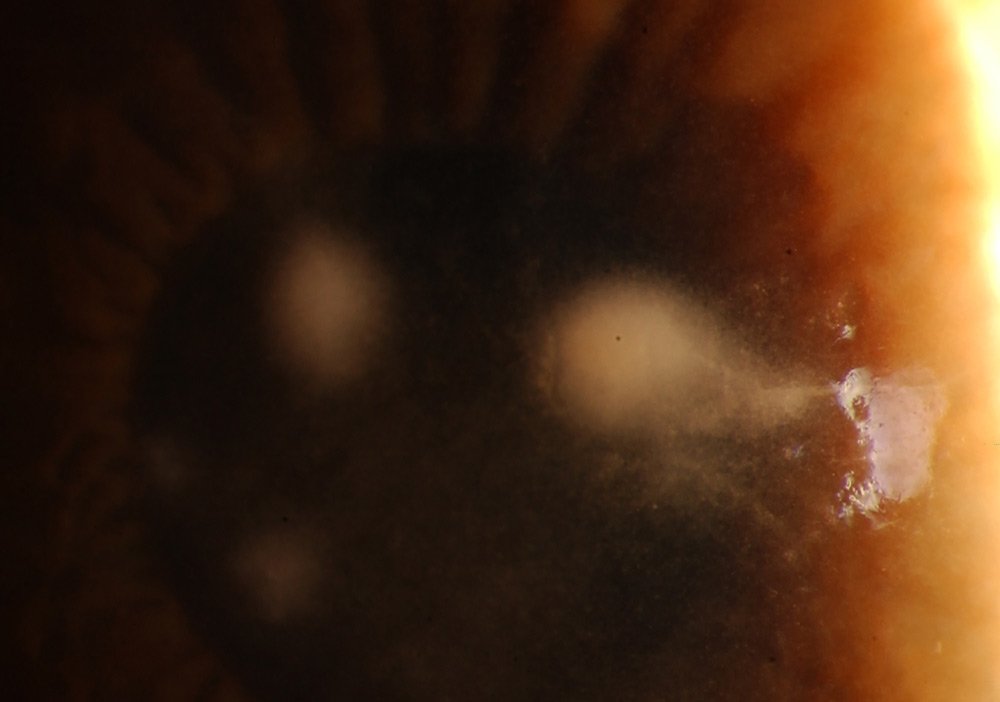
Source: Francis I. Proctor Foundation
Dr. Seitzman also noted PCR as a helpful molecular diagnostic tool, but she said it requires the physician to “guess” the target organism. “Primers are only used against the virus we ordered,” she said. “Here, false negatives are common if the wrong test is ordered. For example, if our patient had VZV keratitis, and we only ordered HSV PCR, we would miss learning the etiology. This is one reason why unbiased or ‘hypothesis-free’ tools like metagenomic deep sequencing are so exciting.” Dr. Seitzman further noted that working with her colleague, uveitis specialist and geneticist Thuy Doan, MD, PhD, they’ve shown that metagenomic deep sequencing can reliably detect unexpected, fastidious, and atypical organisms in corneal samples.
Dr. Tuli stressed that contacts lenses and contact lens hygiene are a big risk factor for many unusual corneal infections. Sleeping in, showering in, and swimming in contacts, not cleaning them, and buying them from non-traditional sources are possible sources for an increased risk of all infections, but especially Acanthamoeba and fungus.
Dr. Seitzman agreed that contact lens wear and water exposure are risk factors, particularly raising suspicion for Acanthamoeba. Any contact lens wearer diagnosed with HSV keratitis should be assumed to have Acanthamoeba first. “Post-surgical wounds, including LASIK flaps or corneal graft incisions, can harbor atypical mycobacteria,” Dr. Seitzman said. “Agricultural trauma is a risk factor for fungal and nocardial infections, and of course, immunocompromised patients are more susceptible to atypical infections in general.”

Source: Francis I. Proctor Foundation
Treatment depends entirely on the organism, Dr. Seitzman said. Acanthamoeba requires prolonged topical anti-amoebic therapy. Atypical mycobacterial infections often need combined topical and systemic antibiotics. In general, antimicrobial susceptibility testing is recommended to guide the treatment of atypical mycobacteria, she said. Triple therapy is commonly recommended. If susceptible, common topical treatments include amikacin, fluoroquinolones, and clarithromycin.
Pythium can be very challenging to treat, Dr. Seitzman said. Topical linezolid and topical azithromycin are common first-line treatments with surgery commonly required for non-responders. “Because these infections tend to present late and are more severe at diagnosis, the treatment courses are longer and the outcomes less predictable compared to typical bacterial keratitis,” she said.
Dr. Seitzman reiterated that atypical infections often require long treatment courses. Acanthamoeba therapy, for example, has a mean treatment course of 4–6 months and even longer in severe cases. Atypical mycobacteria also require extended therapy, with no well-defined clinical guidelines. “Treatment is individualized based on organism, sensitivities, and ocular surface comorbidities,” she said. “Resolution is possible, but many patients are left with corneal scarring or need surgical intervention.”
Moving forward
Dr. Tuli said that a new drug for Acanthamoeba has been approved in the E.U., PHMB 0.08%. She added that some studies have shown that crosslinking either with riboflavin with UV light or rose bengal with green light may help with Acanthamoeba and fungus, as well as atypical infections. Studies are still ongoing.
Dr. Tuli stressed that having a high index of suspicion is important in cases that are not responding to treatment as expected or have unusual appearance. She also noted the importance of culturing all larger or central ulcers, so that if there is an unusual organism it is picked up, and she recommended physicians become familiar with the ancillary treatment modalities, such as intrastromal injections.
Dr. Seitzman is most excited about the advances in diagnostics, particularly metagenomic deep sequencing, which allows for the detection of organisms without prespecifying a target. On the therapeutic side, there is ongoing interest in novel anti-amoebic agents and immunomodulatory approaches, but most new strategies for atypical keratitis are still at the investigational stage.
“The most important takeaway is that ‘atypical’ depends on your environment,” Dr. Seitzman said. “Routinely culturing and keeping track of your local epidemiology is critical, and when you see an infection that worsens despite standard empiric therapy, always keep atypical organisms in mind.”
About the physicians
Gerami Seitzman, MD
Professor and Medical Director
Francis I. Proctor Foundation for Research in Ophthalmology
University of California, San Francisco
San Francisco, California
Sonal Tuli, MD, MEd, MBA
Professor and Chair
Department of Ophthalmology
University of Florida
Gainesville, Florida
Relevant disclosures
Seitzman: None
Tuli: None
Contact
Seitzman: Gerami.Seitzman@ucsf.edu
Tuli: stuli@UFL.EDU