Dry Eye and Ocular Surface Disease Bonus Issue
October 2025
by Liz Hillman
Editorial Co-Director
The importance of the tear film cannot be overstated. As Vance Thompson, MD, EyeWorld Refractive Editorial Board member, says to patients, “the tear lens is 2–4 times more powerful than the implant I’m going to put in your eye.” He tells his patients that the tear film is like “the blood of our cornea” and that it’s the “best anti-red, anti-itch drop there is … and we want more of it.” While ophthalmologists look at the tear film as a therapeutic issue, Dr. Thompson says it’s equally an optical one.
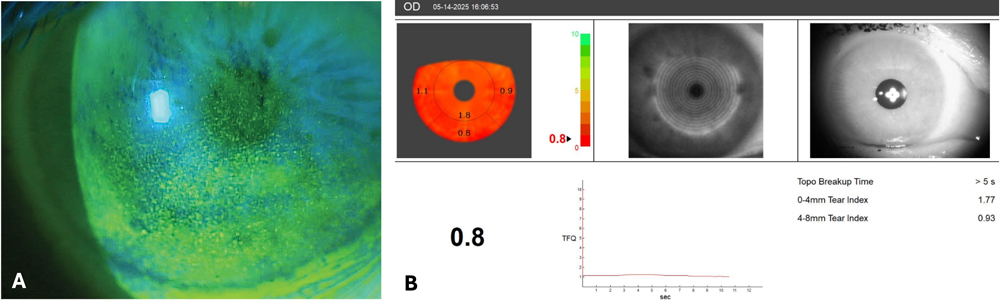
Source: Victoria Fernandes, MD, cornea research fellow, Medical University of South Carolina
Larissa Gouvea, MD, PhD, said the importance and contribution of the tear film to the optical system is not given the attention it’s due. “While surgeons using premium and presbyopia-correcting IOLs are more mindful of the contributions of the tear film to optical quality, it is still underweighted in many preop workflows,” Dr. Gouvea said. “This leads to avoidable postoperative dissatisfaction. However, more often we have seen the literature give more importance to the ocular surface, and I think this is key to improving our understanding of the tear film optics and improving our outcomes.”
George O. Waring IV, MD, FACS, thinks that while the contributions of the tear film to the optical system are appreciated by eye surgeons, it’s poorly understood in the general population. “There’s a wonderful opportunity for education of the public of the importance of a healthy ocular surface,” Dr. Waring said. “The vast majority of our patient population presents with dry eye of some form. Not only is there an opportunity to educate the general population on the importance of the tear film and a healthy ocular service as it relates to visual function but also in terms of the prevalence of dry eye and the etiology of dry eye.”
An abnormal tear film can cause foreign body sensation, fluctuating vision, contact lens intolerance (Dr. Waring noted that contact lens use also contributes to an abnormal tear film), poor quality of vision, and inaccurate IOL power calculations, to name a few. Dr. Waring said many patients are surprised when they’re diagnosed with dry eye.
“We have not done a good enough job educating the public on what the most common symptoms of dry eye are,” he said. “Historically, I think that the dogma has been that your eyes hurt or the eyes feel dry, but we think that the most common symptom, which is often overlooked, is vision fluctuation.”
He said an example of this is the patient who wakes up in the morning and tries to read their phone but can’t see clearly until they blink several times. Similarly, after a long day at work, Dr. Waring said patients like this can’t adequately see the TV without blinking several times. Dr. Waring said he experienced this transient vision himself a few years ago. He, Dr. Gouvea, and colleagues studied it, performing double-pass wavefront on a series of patients with various stages of dry eye.1 They observed and published a correlation between retinal image quality and dry eye severity.
“Often those patients will be 20/20 in clinic but complaining they can’t see well,” Dr. Gouvea said. If that’s the case, understanding the contribution that the tear film is causing to optical quality issues is paramount, especially before proceeding with cataract or refractive surgery.
To assess the impact the tear film might be having on a patient’s optical quality, Dr. Gouvea said she starts with a targeted history and symptom scales, such as the SPEED questionnaire. “At the slit lamp, I always assess tear meniscus height and tear breakup time. Corneal staining and lid margin is extremely important as well. Lid margin disease is known to cause dry eye disease, and significant staining can impact quality of vision,” she said.
Dr. Gouvea will also conduct tear film analysis with the iTrace (Tracey Technologies) to determine tear film quality. “I think this is a good tool to show our patients how their vision is being affected. I have previously used the Keratograph 5M [Oculus], another comprehensive device that helps document non-invasive tear breakup time, and meibography. These are essential for patients’ understanding of their disease and can even improve adherence to treatment,” Dr. Gouvea said. She has also previously used the HD Analyzer (Visiometrics).
Dr. Waring said the HD Analyzer is more of a research tool and is currently not widely used, but he finds the iTrace ray tracing technology very effective in its ability to objectively evaluate dry eye. He also uses the Pentacam AXL Wave (Oculus) for high-resolution tomography pattern analysis, which can be “highly suggestive of dry eye objectively,” and meibography with LipiFlow (Johnson & Johnson Vision) to evaluate structural changes in the meibomian glands. Like Dr. Gouvea, Dr. Waring looks for signs of chronicity at the slit lamp.
Even if a practice doesn’t invest in all of these diagnostic technologies, Dr. Waring considers tomography a must-have. He said Placido topography is also underutilized for dry eye evaluation and diagnosis. “Most ophthalmologists have access to either Placido-based topography or Scheimpflug tomography of some sort. … These can be very useful diagnostic devices for dry eye. They do not provide functional information, but they give objective information.”
Once it is determined the patient has tear film quality issues that are impacting their optical quality, Dr. Gouvea said she recommends several things—first, improved diet and water intake, warm compresses, and lid hygiene. For drops, she’ll start preservative-free tears. If those don’t work, she’ll prescribe a short-course of steroid and cyclosporine. “I also consider in-office therapies such as thermal pulsation, IPL, or BlephEx. For refractory or very severe patients, I add autologous serum tears or platelet rich plasma,” she said.
Dr. Gouvea said she sees tear film instability as chronic and likely to relapse, so she rarely considers patients “done” with treatment. If patients are not having cataract or refractive surgery, she de-escalates therapy to maintenance mode where their symptoms are controlled and the surface is stable. “I explain they will always need to do something to make sure their symptoms are under control—warm compresses/lid hygiene at least once a day and some sort of artificial tears,” she said, noting that some patients will require ongoing anti-inflammatories.
If she is planning for surgery, Dr. Gouvea sees a patient as accomplishing control when their metrics are stable on at least two visits.
The approach to tear film instability in Dr. Waring’s practice is two-fold. He said there is an emphasis on addressing the underlying root cause, such as contact lens overuse, Demodex, or rosacea blepharitis. Then the focus shifts to ocular surface optimization. “If [the ocular surface is] more severe, we’ll work on it in advance of vision correction, but it’s part of a holistic program that we outline in our preoperative consultation.”
Dr. Waring also said that maintaining the tear film is an enduring process. He said it’s important to address the root cause of the problem, particularly if the dry eye may be affecting their preoperative measurements. However, maintaining a healthy ocular surface is not one and done—it’s ongoing.
“The tear film’s contribution to the optical system is not only important, it’s the most important of the optical surfaces of the human eye,” Dr. Waring said. “We are vision correction specialists on all optical surfaces. Whether it’s the front of the cornea, the back of the cornea, crystalline lens, at every surface, we have a solution. But we can’t disregard the most important surface, which is the ocular surface. We have recently described this as improving ‘visual performance,’ and we think this is the true opportunity to optimize visual performance.”
About the physicians
Larissa Gouvea, MD, PhD
Assistant Professor of Ophthalmology
Storm Eye Institute
Medical University of South Carolina
Charleston, South Carolina
George O. Waring IV, MD, FACS
Waring Vision Institute
Mt. Pleasant, South Carolina
Reference
- Gouvea L, et al. Objective assessment of optical quality in dry eye disease using a double-pass imaging system. Clin Ophthalmol. 2019;13:1991–1996.
Relevant disclosures
Gouvea: None
Waring: Johnson & Johnson Vision, Oculus, Tracey Technologies, Visiometrics
Contact
Gouvea: gouvea@musc.edu
Waring: georgewaringiv@gmail.com


