Refractive: Lessons learned
December 2023
by Liz Hillman
Editorial Co-Director
The rotational stability of toric IOLs and reposition rates have been well studied and reported. In most cases (95% according to one study1), any rotation that occurs postop is usually 5 degrees off axis or less.
Brandon Baartman, MD, reported a similar rate of toric rotation requiring intervention. David R. Hardten, MD, said less than 1% of his toric IOL cases need rotation. Bryan Lee, MD, JD, also reported a less than 1% return-to-OR rate for toric IOLs.
“With modern lens design, it’s not all that common of an occurrence that an IOL will appear to be ‘off axis’ postoperatively, where the lens power axis and corneal cylinder are misaligned,” Dr. Baartman said.
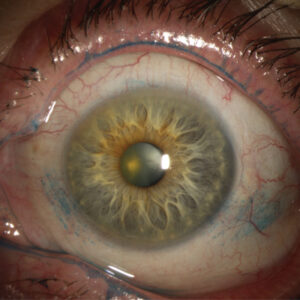
Source: David R. Hardten, MD
Prevention
To avoid residual astigmatism in the first place, Dr. Baartman said he makes sure to use up-to-date calculators, like the Barrett Toric Calculator, and Placido disc topography.
“I mark the eye preoperatively to account for cyclorotation and will use an intraoperative ring (e.g., Mendez toric marker) to make sure my alignment is correct. There are a number of image guidance systems out there that do a lot of this work for surgeons, and I personally like having the ORA intraoperative aberrometer [Alcon] to confirm axis of astigmatism,” Dr. Baartman said.
Dr. Baartman said there are a few things surgeons can do to reduce the risk of in-the-bag IOL rotation postop: 1) ensure 360 degrees of overlap of the anterior capsule with the optic, 2) leave the anterior capsule unpolished, 3) remove all viscoelastic, and 4) leave the eye slightly hypotensive. He added that in long eyes (those with an axial length of more than 28 mm), surgeons can consider placing a capsular tension ring to redistribute tension and encourage sufficient contact with the lens implant to prevent rotation.
Dr. Hardten also discussed methods to ensure correct initial alignment (marking the 3 o’clock and 9 o’clock position while the patient is sitting upright, looking for a vessel, pinguecula, or other unique characteristic in the eye, and topography) and techniques to help the IOL stay where it’s placed. He said to completely allow the IOL to unfold, remove all the viscoelastic (especially under the IOL), and use careful wound construction to keep the eye at physiologic pressure after surgery. Like Dr. Baartman, Dr. Hardten said he uses a capsular tension ring in larger eyes.
Dr. Lee uses a digital marking system, which he noted has been shown to improve toric outcomes compared to manual marking. He also uses intraoperative aberrometry and if he is using dispersive viscoelastic, removes it from the eye and switches to cohesive prior to aberrometry. He’ll then remove all the viscoelastic, going behind the optic with the I/A.
“I gently bump the IOL against the posterior capsule before putting in intracameral antibiotic, and I tell the patient not to squeeze as I remove the speculum and to let the OR chair do the work of sitting up,” Dr. Lee said. “We ask patients to restrict bending, lifting, straining, and eye rubbing and to avoid close activities such as reading, cell phone use, and computer use for 24 hours.”
Even with perfect surgery, calculations, and placement, malpositioning still occurs. Intraoperatively, this is usually due to incorrect data acquisition (incorrect estimation of axis of astigmatism) or misjudged cyclorotation. Dagny Zhu, MD, said it can occur in the early postop days because the capsule hasn’t contracted enough to hold the IOL in place. If rotation were to occur later, it is more likely due to trauma, Dr. Zhu said.
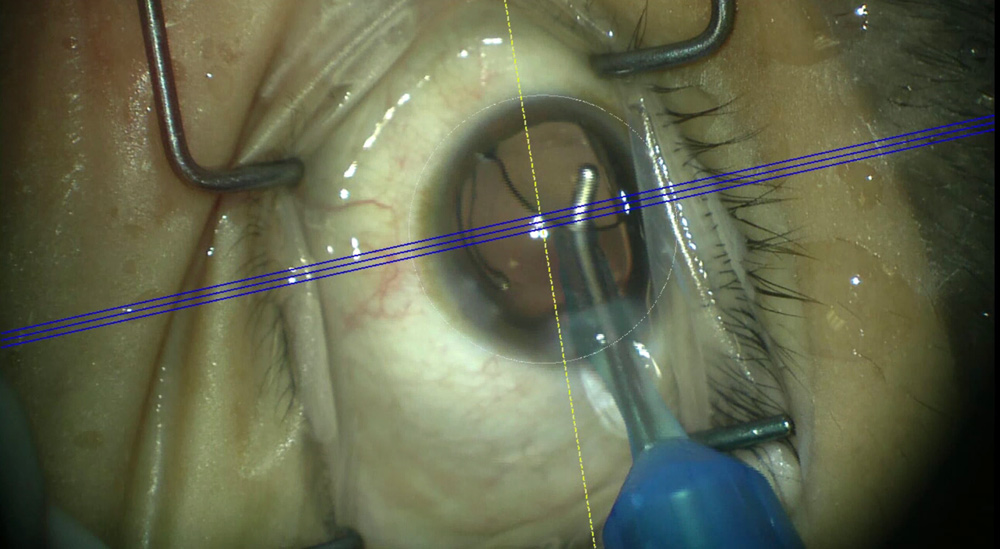
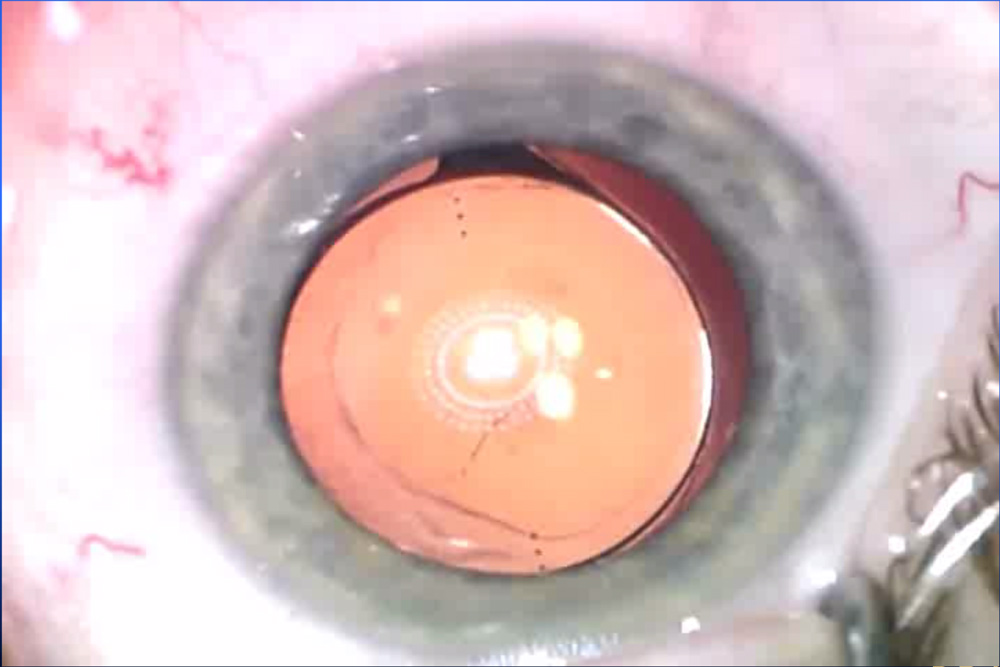
Source: Bryan Lee, MD, JD
Management
When it comes to residual astigmatism, Dr. Lee said it’s important to distinguish between incorrect axis due to the surgical plan vs. IOL rotation. Unreliable biometry and unrecognized corneal factors could mean the chosen toric power or axis were suboptimal, so treating the ocular surface and remeasuring may be helpful. Dr. Lee said there used to be a large difference in postoperative toric IOL stability among manufacturers, but this has significantly improved.
Dr. Baartman said most cases of rotation occur early in the postop period, and it’s often the patient notifying the surgeon that something seems off.
“The earlier these patients are evaluated and refracted if UCVA does not meet expectations, the earlier you can identify malposition,” he said. “For the sake of optimal patient satisfaction, I think it’s best to identify and address the problem as early as possible.”
If unexpected residual refractive error is detected in toric IOL patients (whether it’s a monofocal, EDOF, or multifocal), Dr. Baartman said the evaluation starts at the slit lamp.
“Proper slit lamp measurement of the current rotational position is critical, and it’s also important to ensure the lens implant is centered in the bag with proper anterior capsular overlap and that neither haptic has found its way into the sulcus,” Dr. Baartman said. “If the intraoperative position was documented at the end of the case, you’ll know which direction the lens needs to be rotated in and by how much. You can use an astigmatism calculator like astigmatismfix.com.”
If rotation is necessary, Dr. Baartman said he’ll bring patients back within a week, reopen the primary incision, and insert just enough cohesive viscoelastic to free up and rotate the lens. If residual refractive error is recognized a month or more postop, Dr. Baartman said he’ll usually use a laser refractive procedure to correct it.
Dr. Lee recommended waiting about 2 weeks to allow the capsule to tighten before going back in to rotate.
“This has been shown to reduce re-rotation. There are different calculators to help determine the ideal axis of the toric IOL based on the IOL power, position, and postoperative refraction,” he said. “Assuming the IOL power is OK and that it doesn’t need to be exchanged, we will usually be able to rotate the IOL using balanced salt solution on a cannula, trying to open the capsule as little as possible.”
Dr. Zhu said patients with true IOL rotation often had 20/20 vision on their first day postop, but it dropped in the subsequent week or two. She said she’s honest with these patients, telling them that while it looks like the lens moved, the good news is it can be fixed. Dr. Zhu is able to perform office-based surgery, so she can take the patient back and rotate the IOL on the same day it’s identified. She also noted that if the cornea is healthy enough and if the patient doesn’t want to go back inside their eye, she’ll offer LASIK or PRK.
“Laser vision correction is also a good option when you have a patient in whom residual refractive error is not completely explained by IOL rotation, where the calculations might be off or the wound is affecting the final astigmatism,” she said.
Sometimes the issue isn’t IOL alignment but changes in corneal curvature postop. This can occur from wound contraction and scarring or relaxation, Dr. Hardten said. While most IOL calculators take into consideration posterior corneal astigmatism, it’s also a possible source of residual refractive error because it’s a difficult area to measure, he said.
ARTICLE SIDEBAR
Lessons learned
Dr. Baartman: I think early identification and intervention of postoperative problems is always a worthwhile pursuit, particularly if dealing with a refractive cataract patient with unexpected outcomes. They have usually paid out of pocket for their outcome, and they’re going to want to know you’re invested in their success. It’s nice when you have staff check in on patients as they go through the healing process, especially if they’d traveled a distance for surgery and may be doing their postoperative care elsewhere.
Dr. Hardten: One of the main lessons I’ve learned over time for astigmatism correction is to utilize toric IOLs for regular astigmatism. There have been some reports of using torics for keratoconus, post-RK, or post-PRK/LASIK, but these are very difficult cases, and it’s likely that leaving the astigmatism alone, or considering astigmatic keratotomy in non-ectatic eyes and later PRK, is more useful.
Dr. Lee: Although toric IOLs can rotate, the rate is very low, and the success rate for repositioning is very high. Correcting astigmatism is so advantageous for patients that I don’t think rotation is something to fear.
About the physicians
Brandon Baartman, MD
Vance Thompson Vision
Omaha, Nebraska
David R. Hardten, MD
Minnesota Eye Consultants
Minnetonka, Minnesota
Bryan Lee, MD, JD
Altos Eye Physicians
Los Altos, California
Dagny Zhu, MD
NVISION Eye Centers
Rowland Heights, California
Reference
- Singh A, et al. Rotational stability of toric intraocular lenses. Med J Armed Forces India. 2022;78:68–73.
Relevant disclosures
Baartman: None
Hardten: astigmatismfix.com
Lee: None
Zhu: None
Contact
Baartman: brandon.baartman@vancethompsonvision.com
Hardten: drhardten@mneye.com
Lee: bryan@bryanlee.pro
Zhu: dagny.zhu@gmail.com