Refractive: Lessons learned
December 2023
by Ellen Stodola
Editorial Co-Director
Many surgeons have now gained experience with the EVO ICL (STAAR Surgical), which was FDA approved in April 2022. Several spoke to EyeWorld about what they’ve learned from using it in practice.

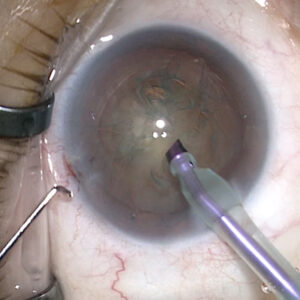
Source: Arjan Hura, MD
Many physicians were using ICLs as a resource prior to the EVO ICL’s approval. Gregory Parkhurst, MD, has been a long-time ICL user, so he’s familiar with the platform. “Using the ICL as an important part of our refractive surgery offerings isn’t a new thing for us,” he said. “But when I speak to colleagues and peers, a lot are starting to try the ICL again now that the EVO ICL has been approved. Maybe they tried it years ago and stopped, and now they’re taking a second look. In our case, it’s the next modification of a platform that we’ve been using all this time.”
While Dr. Parkhurst didn’t notice any major changes when the EVO ICL got approved, he did say that he was surprised at how much growth his practice has seen in ICL use since the approval. “I expected we might see a few more patients who qualified for it than who had qualified before, but I didn’t expect it to have the dramatic impact that we’ve seen,” he said. “More patients are asking about it, more are getting referred for it,” he said, adding that efficiencies on the operational side are also making it easier to get a patient through the process.
Arjan Hura, MD, is a refractive surgeon at the Maloney-Shamie Vision Institute and said that he utilizes the EVO ICL on an almost weekly basis, and like Dr. Parkhurst, his practice has seen a dramatic increase in volume since the approval of the EVO ICL. Similar to other refractive surgeons, prior to the FDA approval, he was routinely implanting ICLs with his first experience in his refractive surgery fellowship in Cleveland, Ohio.
Amy Lin, MD, said she has also used ICLs for years. “I didn’t change anything that I was doing as far as marketing more because I was already doing ICLs,” she said. “But I did find that because of the launch of the EVO ICL, there was more press about it, so I had more patients coming in asking about it.”
Dr. Lin thinks the EVO ICL is a great option for high myopes and those with moderate myopia who are not candidates for LASIK or PRK due to thin corneas. “It’s great to be able to offer something for those patients instead of telling them they’re not candidates for laser vision correction,” she said.

Source: Alexandra Wiechmann, OD
As far as who to present it to, Dr. Parkhurst separates this into categories. The first, he said, are the lowest hanging fruit, or patients who come in seeking refractive surgery, and for one reason or another, they aren’t suitable candidates for laser vision correction. This could be because the magnitude of their myopia is very high, the cornea is very thin, or there’s something abnormal about the cornea, he said. “Those are the candidates in whom you can deliver the outcome the patient is seeking, which is to see without glasses or contacts, but we’re doing so in a way that doesn’t touch the cornea and doesn’t increase ectasia risk.”
The second category, he said, is the group of patients who could otherwise have laser vision correction but want to hear about an alternative. They are interested in learning about the pluses and minuses of having refractive surgery by phakic IOL instead of laser vision correction. “[In] that category, we make sure there’s a lot of education and communication with the patient as early in the experience as possible,” he said. “When they call, our engagement center mentions that there’s more than one way to do this … so when they arrive at the practice, they’re not surprised at the possibility of hearing about different options; as they go through the consultation process, we tell them all the various procedures they’re a candidate for, including the EVO ICL when that’s the case.”
He will judge patients’ response to this non-laser vision correction method. Some people will want to know more, and some may be fearful of something that they haven’t heard of before. If they’re open to hearing more, we continue to educate them, he said. “Some will choose the EVO ICL even if they’re a perfectly good candidate for laser vision correction.”
Dr. Lin said that it’s a big advantage not having to do a peripheral iridotomy. “Before the EVO ICL, I would do an intraoperative peripheral iridotomy at the time of ICL surgery,” she said, adding that not having to perform iridotomies now helps save time in the OR. “I think patients also like the fact that they’re not getting an iridotomy, so not having that extra step is nice.”

Source: Alexandra Wiechmann, OD
Dr. Parkhurst agreed that it’s a big advantage to not have to do the iridotomy before implantation. “That’s made the whole process in terms of the number of appointments, scheduling, and logistics simpler,” he said.
When teaching fellows, he said they would occasionally see IOP spikes in patients having ICL procedures prior to the EVO ICL getting FDA approval. But since he began using the EVO ICL, there have been zero instances of this. “There have been no cases where we’ve had to come in to deal with an IOP spike on the night of surgery,” Dr. Parkhurst said. “We’re confident offering this technology.”
Dr. Hura has also noticed the decreased incidence of postop IOP issues. “The EVO ICL has a central port, as well as four peripheral ports, that allow for constant flow of aqueous humor through the ICL. Based on the 10-year international data, this has led to a near zero incidence of significant postoperative IOP issues and early cataract formation,” he said.
He also noted that obviating the peripheral iridotomy is a major advancement for patient comfort and the overall surgical experience. Peripheral iridotomies are a permanent alteration of iris tissue and sometimes had to be enlarged if initially too small and were sometimes a source of dysphotopsias. Although the EVO ICL can still result in some dysphotopsias, not having to remove iris tissue is a great benefit to the latest iteration of ICL technology, he said. “Additionally, the flow of aqueous humor through the ICL ports theoretically could lead to a buffer zone when it comes to ICL sizing,” Dr. Hura said. “As a surgeon, I would love to see more ICL sizes and an expanded range of refractive error that can be corrected [in the United States].”

Source: Alexandra Wiechmann, OD
Dr. Hura noted that while complications are rare, there are some possible issues that can arise, including postoperative rotation of a toric ICL or a vault that is too shallow or too large. These are issues that are easily remedied in the hands of a skilled refractive surgeon, he said.
Dr. Lin noted that patients still complain of glare and halos, though they may not be as bad as with the prior version of the ICL. “It’s still something that’s almost universally noticed by patients,” she said. “One thing that I learned after I put in my first EVO ICLs is that the glare and halos persist even beyond a month.” For this reason, Dr. Lin said it’s important to explain to patients that these will likely be an issue. The overwhelming response is that patients are still very happy with their ICLs despite the glare and halos, she said.
While Dr. Lin doesn’t have any specific contraindications for using the EVO ICL, she noted that she does see occasional cases of oversized ICLs, despite all the different ways she is measuring white to white (including UBM). This issue was something that she also noticed in the previous ICLs as well. “I’ve had some cases of the ICL being over vaulted,” she said. “I’ve been trying to use slightly smaller ICLs than the ones recommended by the nomogram.” Dr. Lin noted that she does not do bilateral, same-day ICLs because if there is an over vaulted ICL, she will use a smaller size for the second eye.
Dr. Parkhurst agreed that sizing strategy is extremely important for success with ICLs. “We’ve got some new nomograms we’re working on, with artificial intelligence and machine learning, to use diagnostic scans to predict the ideal size for the ICL,” he said. “One of the most critical things in terms of having success is picking the size right, and it’s nuanced. It’s not easy in the current state without the right diagnostic technology to size the lens properly. Because we’re now confident with the way we’re doing sizing with UBM technology and arc scans, we’re finding that we’re able to go to shallower anterior chamber depths than what we used to be comfortable with.” For example, he said the minimum AC depth before the EVO ICL was 2.8 mm, but now he has even gone to 2.6 mm. “That is one area where we’re finding that more patients qualify, whereas we would have turned them away in the past,” he said. Dr. Parkhurst added that he wouldn’t recommend surgeons new to the EVO ICL going this low in their first handful of cases until they are confident in their sizing strategy.
ARTICLE SIDEBAR
Lessons learned with Dr. Hura
- Multiple biometers and imaging modalities can help with ICL sizing, and utilizing different sizing nomograms can be beneficial in making a decision for cases that fall between two different sizes.
- Just as with IOLs, it is important to be able to explant an ICL if implanting one.
- Don’t rush at the end of a case, and take time to thoroughly remove as much OVD as possible.
- Analyze your refractive outcomes and vaults to refine your sizing and power selection.
About the physicians
Arjan Hura, MD
Maloney-Shamie Vision Institute
Los Angeles, California
Amy Lin, MD
Associate Professor of Ophthalmology
John A. Moran Eye Center
University of Utah
Salt Lake City, Utah
Gregory Parkhurst, MD
Parkhurst NuVision
San Antonio, Texas
Relevant disclosures
Hura: STAAR Surgical
Lin: None
Parkhurst: STAAR Surgical
Contact
Hura: arjan.hura@gmail.com
Lin: amylin78@gmail.com
Parkhurst: gparkhurst@parkhurstnuvision.com