Cataract: Lessons learned
December 2023
by Ellen Stodola
Editorial Co-Director
Before deciding to move forward with cataract surgery, there are a variety of factors that surgeons must consider. Several physicians discussed the timing of the surgery and how they counsel patients about this.

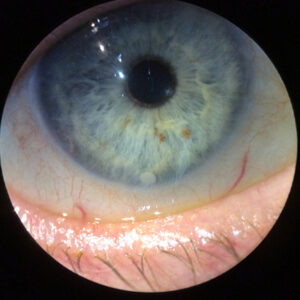
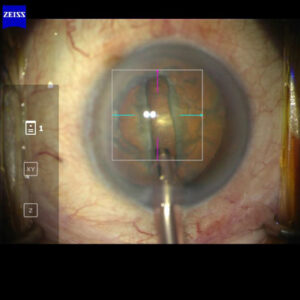
Source: Rom Kandavel, MD
Mitra Nejad, MD, said it’s less about how advanced the cataract is on the exam and more about the patient’s description of how they are bothered by their vision. Dr. Nejad has a mix of patients, including referrals from colleagues, so she often sees more visually significant cataracts that are ready for surgery. “On the other hand, I’ll get some self-referrals or primary care physician referrals for evaluation of cataract, and I often schedule those alongside an optometrist who I work closely with, in case all they need is an updated glasses prescription,” she said. When getting referrals from retina colleagues, Dr. Nejad said these might need to be operated on more quickly because the cataract is impairing the physician’s ability to provide treatment for the retina pathology.
Dr. Nejad said it’s rare that the cataract surgery must happen urgently. However, she noted that some patients come in having failed a driving test, and she wants to address these patients as soon as possible to get them back to functional status. “Otherwise, I usually tell the patient, ‘The cataract is significant, I think you should consider surgery, but the good news is there’s nothing urgent about it, and you can schedule the surgery at your convenience.’” If the cataract is mild and the patient isn’t eager to do surgery, Dr. Nejad will ask the patient to come back in a year. If the cataract is dense and the patient isn’t eager to have surgery, she’ll have them return sooner. Dr. Nejad has noticed that because patients are hearing good things from family and friends about refractive cataract surgery, this decreases their overall anxiety about eye surgery.
Dr. Nejad noted that she has seen a wave of worse pathology with the COVID-19 pandemic because patients have gotten used to a lifestyle with less driving and more time at home. Patients weren’t coming in for elective procedures and weren’t noticing visual impairment as much until they had to go out and drive at night again. “For a while, I was seeing a lot of advanced cataracts, a lot of people who waited longer than they should have,” she said.
Amandeep Rai, MD, has also found that coming out of the pandemic, there has been a noticeable trend toward patients presenting with more advanced cataracts. “The delayed access has certainly resulted in more patients presenting with advanced, visually significant cataracts in the last 2 years,” he said. “However, I do see a fair number of patients with milder symptoms who are referred from their optometrist for a surgical consult,” he said. “If they are minimally symptomatic, I will often ask them to follow up with the optometrist until the cataract becomes more advanced.”
The decision to proceed with cataract surgery is jointly made by the patient and the ophthalmologist, Dr. Rai said. While cataract surgery is safe and can have a profound impact on a patient’s quality of life, it is ultimately an elective surgery. With more advanced cataracts, the patient has already been symptomatic for some time and arrives at the consultation ready to proceed with surgery.
“With respect to allowing the cataract to become more visually significant, the Lens Opacities Classification System III (LOCS III) is a great scale. With the most common subtypes of cataracts, a lower LOCS III grade cataract can be observed if the patient is tolerating the lens changes, while a higher grade cataract is ready for surgery,” he said. “If we elect to observe a cataract, I ask the patient to monitor their symptoms and return once they think their lifestyle is impacted. Typical early complaints include difficulty with night driving or frequently updating their spectacles due to shifting refraction and a drop in their best corrected visual acuity.”
Rom Kandavel, MD, thinks that as a patient, a good question to ask when considering cataract surgery is, “With my best pair of glasses, what vision problem do I wish to solve through cataract surgery?” As a surgeon, you may want to ask, “Is the vision limiting the patient’s quality of life or their ability to perform daily activities the way they want to be perform?” If you can’t find the answer to those questions, you probably shouldn’t be operating on that patient, he said. “That is the premise of what I look for in a conversation. It’s not a discovery when they need surgery. The vision is already impacting the patient’s quality of life. The need to improve the vision should be obvious to the surgeon and to the patient.” You never want to be in a position where you’re telling the patient that they have a problem that they are unaware of. He added, “In the rare circumstance that a patient has a problem after surgery, like glaucoma or retinal detachment, the patient should look back and know they made a clear self-driven decision to improve their vision through surgery.
“Patients will commonly know they are ready for surgery, but they’ll still ask me, ‘Do I need this surgery?’” It’s not because they’re not sure, but Dr. Kandavel said they want reassurance in order to move forward with their decision. He will be supportive and positive. “I never do surgery on someone who I don’t think it will help significantly.”
He also said that as surgeries become more routinely successful, physicians may become less mindful of the potential complications of a procedure. Operating on borderline cases can be less successful. “A good result, when evaluated in the context of moderate preoperative vision impairment, becomes unacceptable with a symptom such as mild halo after surgery.
“I always tell residents that the patient’s satisfaction with your surgery is not always linked to the result but to the process that you establish with the patient, earning trust over years of appointments,” he said. “If you build that trust, not only do you have a more fulfilling career, but you also have a more successful one.” When patients trust you, they are much more likely to put their faith in your recommendations because of that earned relationship.
Dr. Kandavel said there are some reasons to operate sooner rather than later. One potential issue is cases with narrow angles. “In hyperopic patients who fail to have an angle improvement with laser iridotomy, cataract surgery can become medically indicated,” he said. In a discussion of factors that could sway a surgeon or patient to have surgery done sooner, one of the most common is the desire of the patient to reduce spectacle dependence. He often counsels patients, “Don’t do cataract surgery just to eliminate glasses because I cannot ensure that 100% of the time.” However, there are some circumstances where less spectacle dependence can play a role. “If the patient has presbyopia and is a high hyperope or myope who has already undergone vitreous separation, you could consider the desire to reduce spectacle dependence because there is also a significant quality of life improvement in those circumstances.” Another example would be someone who is a long-time contact lens wearer with monovision. Those patients may not tolerate their monovision any longer, which can be unsettling. “If they desire to stay in functioning monovision and they no longer can, cataract surgery may be indicated,” he said. Patients with glaucoma who are on multiple drops and have trouble taking them consistently may be another case in which to operate earlier, when combined with MIGS procedures to improve compliance.
Dr. Rai said patients may present with comorbid conditions that add complexity to their cataract surgery. Common ocular comorbidities include pseudoexfoliation syndrome, previous vitrectomy, and poorly dilating pupils that may predispose to intraoperative floppy iris syndrome. “We know these patients may be at increased risk for intraoperative complications, and allowing the cataract to become hypermature only serves to elevate the complexity of the surgery for the surgeon and the corresponding risk for the patient,” Dr. Rai said.
“I have been referred patients who previously had complicated surgery elsewhere for their first eye, and their second eye was canceled and has subsequently progressed to a hypermature cataract,” Dr. Rai continued. “Understandably, these patients are concerned about proceeding with cataract surgery in their ‘good eye,’ but they have paradoxically increased the risk for complications by delaying surgery. Of course, when there is a surgical complication, the first priority is to rehabilitate that eye to its visual potential, which is often quite good. Once that is accomplished, the other eye should not be ignored, and the patient should be offered cataract surgery in a reasonable timeframe. A referral to a colleague can help reduce stress for both the patient and ophthalmologist. Another example is a patient who presents with a rapid onset white cataract in one eye and an early posterior subcapsular cataract in the other eye. I would proceed with removing both cataracts as soon as possible instead of allowing the mild posterior subcapsular cataract to rapidly progress into a more complicated surgical case.”
When deciding when to move forward with cataract surgery, Dr. Kandavel said he will ask patients to clear their schedules for 3–4 weeks after surgery in case anything occurs in the postop period. “I also tell them on initial consultation that they won’t be able to go in the pool or in the water at the beach. I always tell them if they plan to go outside the continental U.S. to take that trip before they have surgery. I generally don’t recommend doing one eye, going on vacation, and coming back and doing the other,” he said. “I frequently will have a husband and wife come in for a simultaneous consultation, and I always tell them that only one person can have surgery at a time because they need someone to be the driver, and they may need someone to put in drops if that ends up being a problem.” If patients decide at the end of the consultation to postpone surgery, Dr. Kandavel said that he advises them that he will repeat testing and the dilated exam 90 days after the consultation.
“Patients are highly educated about cataract surgery and their lens options even prior to their consultation with me,” Dr. Rai said. “They have consulted their friends and the internet to learn about their intraocular lens options, and many patients are seeing cataract surgery as an opportunity to improve their clarity and best corrected vision and their pre-existing refractive error.
“Patients who have more advanced cataracts are very easy to please because the postoperative difference in best-corrected visual acuity is more appreciable. However, with improved IOLs and biometry, modern cataract surgery allows great predictability with respect to reducing refractive error. As a result, patients who have significant pre-existing refractive error also tend to be quite pleased following cataract surgery as they notice a large benefit in their uncorrected distance visual acuity and possibly a presbyopic benefit as well,” Dr. Rai said.
ARTICLE SIDEBAR
Lessons learned
Rosa Braga-Mele, MD, Cataract Editorial Board member, shared a lesson she has learned to “level up”:
I have found that when dealing with complaints of quality of vision from MFIOL patients, it is important to listen but also show them what their near vision would be like without the MFIOL. I put up –2.50 trial lenses in front of their eyes while having them hold a Jaeger near card. Once they see what their up-close vision would have been like with a monofocal IOL, most will stop complaining about little issues.
Also always let your patients know it can take up to 3–6 months for foreign body sensation to go away and neuroadaptation to take place with their new lenses.
About the physicians
Rom Kandavel, MD
Colvard-Kandavel Eye Center
Encino, California
Mitra Nejad, MD
Assistant Professor of Ophthalmology
David Geffen School of Medicine
University of California, Los Angeles
Los Angeles, California
Amandeep Rai, MD, FRCSC
Residency Program Director
Department of Ophthalmology & Vision Sciences
University of Toronto
Toronto, Canada
Relevant disclosures
Kandavel: Alcon, Bausch + Lomb, Glaukos, Tarsus
Nejad: None
Rai: Alcon, Bausch Health
Contact
Kandavel: valleyeyedoctor@gmail.com
Nejad: MNejad@mednet.ucla.edu
Rai: AmandeepRaiMD@gmail.com