Cornea: Hot topics in ophthalmology
December 2022
by Liz Hillman
Editorial Co-Director
For the last decade, interferon alpha-2b (IFNα-2b) was the preferred pharmacologic therapy for ocular surface squamous neoplasia (OSSN) in the U.S. It was an effective, non-toxic immunotherapy that was comfortable for the patient, said Carol L. Shields, MD, one of the country’s foremost ocular oncologists.
IFNα-2b was not without its drawbacks. It took longer to resolve cases of OSSN, it was unstable, necessitating special handling to maintain its efficacy, and it was expensive. But it was, Dr. Shields said, still “a wonderful drug to treat OSSN.” Then, “in walks COVID-19,” Dr. Shields continued. With the pandemic, the makers of interferon decided they would no longer manufacture it for ocular conditions, transitioning its use for treatment of COVID-19 patients instead.
Now, IFNα-2b for treatment of OSSN is largely unavailable worldwide, though Dr. Shields noted that her colleagues in India say it is still being produced there.
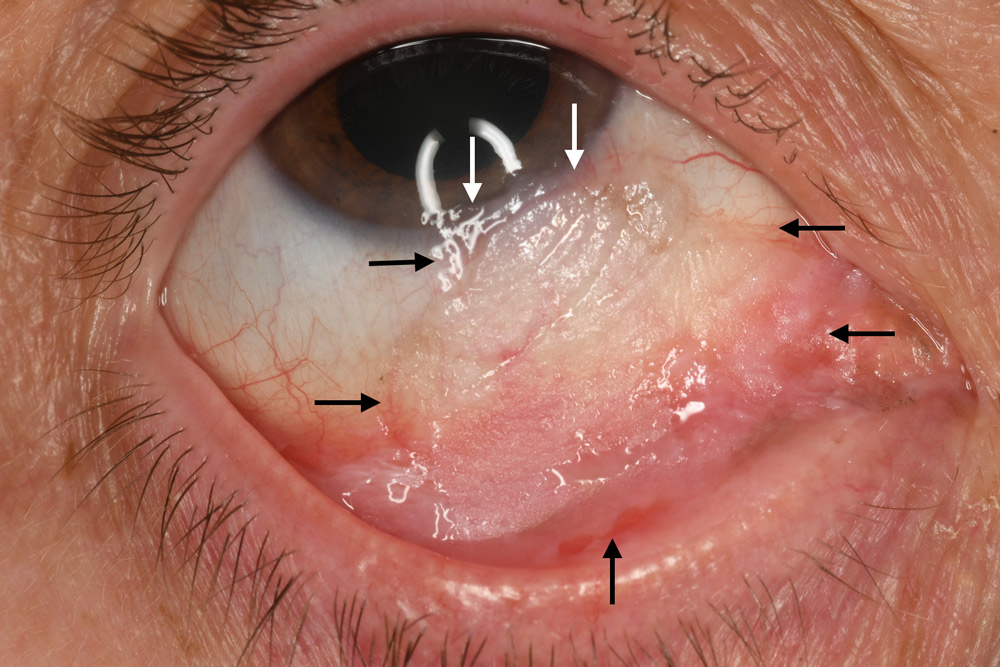
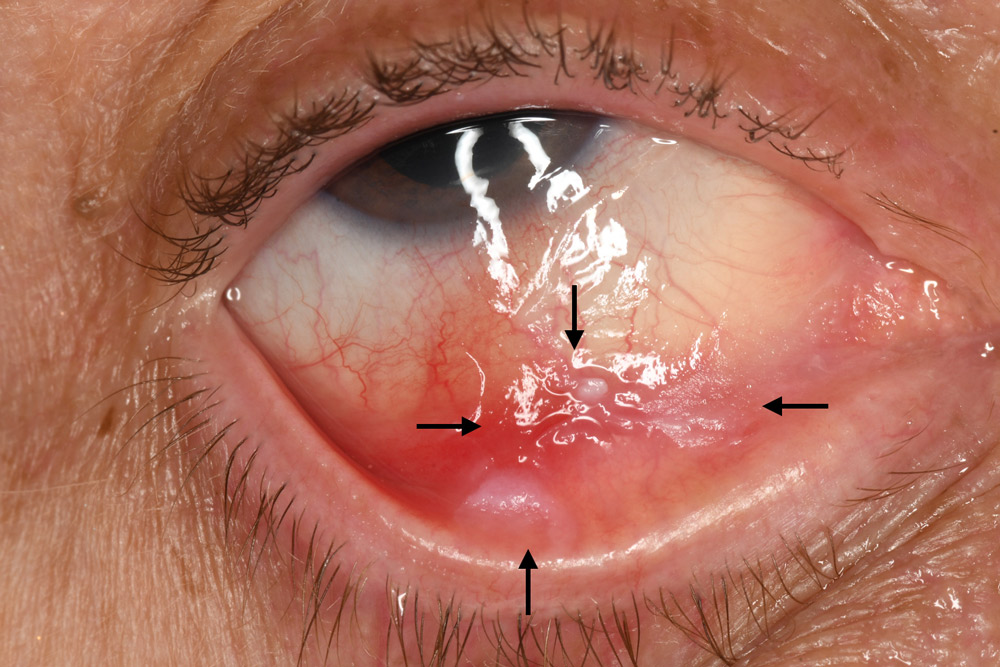
A. Before: The flat neoplastic tumor is extensive (arrows), occupying limbus to near eyelid margin, measuring 25 mm in base.
B. After: Following 1 month of topical 5-FU, the mass has substantially reduced to a smaller basal dimension of 14 mm diameter. After a 1-month drug holiday, another month of 5-FU was planned.
Source: Carol L. Shields, MD
OSSN treatment options
Dr. Shields gave EyeWorld an overview of the treatment options for OSSN. Generally, the first-line treatment for most cases of OSSN is surgical resection.
“Number 1, it’s quick. Number 2, it’s covered by insurance. Number 3, you don’t have to rely on the patient putting a medication into the eye. Number 4, we get pathology. We’re sent patients with all kinds of different diseases, and we want to be sure that OSSN is OSSN because there are other more serious conditions that can look like it,” she said, noting that some of these more serious conditions wouldn’t necessarily respond to pharmacotherapy.
Dr. Shields said the tumor control rate with surgical resection is 95–98%. She mentioned a study that looked at recurrence rates after surgical resection or pharmacotherapy, finding recurrence rates were similar (about 5%).1
If a patient has established OSSN, recurrence, positive margins, a large OSSN of 6 or more clock hours, or is not a surgical candidate, pharmacological therapy is used, Dr. Shields said. When pharmacotherapy was needed, there was a strong preference for IFNα-2b (given both topically and via injection), Dr. Shields said. Despite some of its considerations—it could cost the patient $200–400 out of pocket each month they were on it, and it can’t be shaken or it loses efficacy—Dr. Shields said patients “hugely benefited” from it.
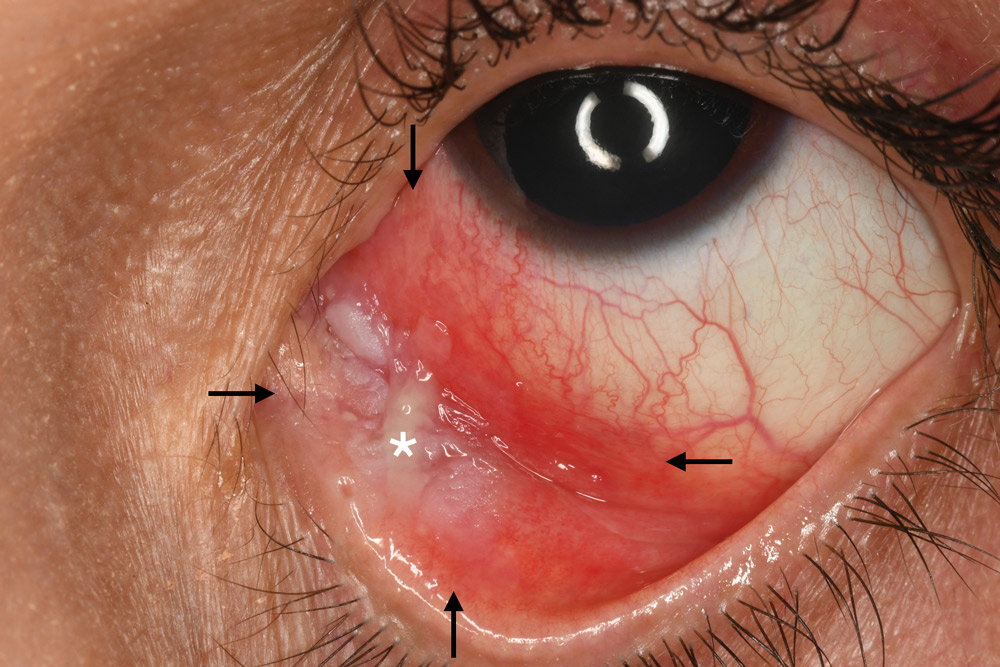

A. Before: The leukoplakia (labeled with *) mass is extensive (arrows), occupying limbus to medial eyelid margin, measuring 30 mm in base.
B. After: Following 2 months of topical 5-FU, with a 1-month drug holiday between doses, the mass completely regressed, leaving no residua.
Source: Carol L. Shields, MD
When interferon became unavailable during the pandemic, physicians treating OSSN were left with alternative pharmacotherapies—topical 5-fluorouracil (5-FU) and mitomycin C (MMC).
“Right now, we’re in a lull where we don’t have interferon, so all of us who treat OSSN are scrambling to find the second best pharmacotherapy, and we think it’s 5-FU,” Dr. Shields said, noting that MMC is more toxic to the epithelial surface and causes complications.
Dr. Shields said that 5-FU and MMC are chemotherapeutic agents where you have to be “100% sure the conjunctiva is sealed” before using them. She said she waits at least a month or two after surgical resection before starting chemotherapeutic agents. If these were to enter the eye, they could cause a scleral or corneal melt. Dr. Shields said that she uses 5-FU 1% but that she knows of other ocular oncologists who use the 0.5% dose with success.
While 5-FU can cause limbal stem cell loss, Dr. Shields said complications are less frequent compared to those that can occur with use of MMC. MMC can cause nasal lacrimal duct occlusion, so many physicians use punctal plugs. The tradeoff is that the MMC can drip on the cheek and can cause periocular redness and scaling, but Dr. Shields said this heals better than eyes with nasolacrimal duct obstruction and chronic epiphora needing reconstruction. MMC still seems to result in an abnormal epithelium with atypical cells. It’s unknown whether these cells are atypical from the MMC or the OSSN.
In general, Dr. Shields said that IFNα-2b can take 3 or so months to resolve OSSN. For a small lesion, 5-FU could take 2 weeks (when used 4 times a day), and larger lesions could take 4 weeks.
“It’s impressive, but usually by the second week patients are calling and saying it’s burning. You have to hold their hand as they’re using it because it’s ‘burning’ the epithelium off the eye,” Dr. Shields said. “I’m very sensitive to OSSN because it is the elderly population. We want quality of life for these people. We don’t want them to have medications that cause tearing, redness, or pain, and that is why interferon was such a great drug. Patients would say each drop was soothing. We had tumors that were gigantic … we would inject these patients and put them on topical, and by the time we finished their course, 3–4 months, it was gone.”
What’s next for interferon
Dr. Shields said when interferon became unavailable in the U.S., the International Society of Ocular Oncology and the American Association of Ophthalmic Oncologists and Pathologists met with the American Academy of Ophthalmology to discuss the situation and possible options.
“There was talk of a company in China … but the cost was out of control. We need an American company to get interested in making interferon because patients hugely benefited from it,” Dr. Shields said. “There is some talk of using alternatives of interferon but there have been no big studies looking at those. There is hope that other types of interferons can be useful, but interferon alpha-2b was well tolerated and effective.”
Dr. Shields said she doesn’t want the ophthalmic community or their patients to worry.
“We have 5-FU. 5-FU is very effective. We had one case of a squamous neoplasia sitting over a glaucoma tube shunt. I didn’t want to operate near that. We put that patient on 5-FU, it melted away, and she’s doing fine,” Dr. Shields said.
Dan Gombos, MD, past president of the American Association of Ophthalmic Oncologists and Pathologists and current president of the International Society of Ocular Oncology, said that the disappearance of IFNα-2b for ophthalmologists has “significantly impacted” physicians’ ability to treat patients. He said that these societies have alerted American and European societies and their colleagues in the field of this issue, but “we haven’t been able to change the access to this medication and that’s where we stand.”
Finding a new company to produce IFNα-2b is ideal, but Dr. Gombos said that won’t be a quick fix for the current situation.
“This is bringing together the ocular oncology community worldwide because many of us are finding … you can’t get the drug; it’s as simple as that,” Dr. Gombos said.
ARTICLE SIDEBAR
History of MMC for OSSN
While MMC is not her preferred first-line therapy, Dr. Shields said its application for OSSN changed the world. She said its use as a pharmacotherapy was discovered by Joseph Frucht-Pery, MD, and Yaacob Rozenman, MD, who published about its success as a topical treatment for patients with squamous neoplasia in 1994.2
“They changed the world with this one innovative thought,” Dr. Shields said. “Back in the 1980s before we had pharmacotherapy, exenterations were done for patients with advanced squamous neoplasia, but now we use pharmacotherapy.”
Dr. Shields said one of her first experiences with MMC for OSSN was in the 1990s in a bilateral case of extensive OSSN treated with wide surgical resection and reconstruction for one eye and with MMC for the other eye.
“It totally cleared up. I have been a believer since then, and I always thank Dr. Frucht-Pery and Dr. Rozenman for their courage and thinking outside the box,” she said.
About the physicians
Dan Gombos, MD, FACS
Professor and Chief
Section of Ophthalmology
Department of Head and Neck Surgery
University of Texas MD Anderson Cancer Center
Houston, Texas
Carol L. Shields, MD
Chief of the Ocular Oncology Service
Wills Eye Hospital
Thomas Jefferson University
Philadelphia, Pennsylvania
References
- Nanji AA, et al. Surgical versus medical treatment of ocular surface squamous neoplasia: a comparison of recurrences and complications. Ophthalmology. 2014;121:994–1000.
- Frucht-Pery J, Rozenman Y. Mitomycin C therapy for corneal intraepithelial neoplasia. Am J Ophthalmol. 1994;117:164–168.
Relevant disclosures
Gombos: None
Shields: None
Contact
Gombos: dgombos@mdanderson.org
Shields: carolshields@gmail.com

