Dry Eye and Ocular Surface Disease Bonus Issue
October 2025
by Ellen Stodola
Editorial Co-Director
As physicians continue to deal with dry eye and ocular surface disease, knowing treatment options that are available and appropriate steps to take for these patients is critical. Several years ago, the ASCRS Cornea Clinical Committee decided to take this on as a primary educational initiative because of lack of awareness and consensus regarding recommendations on ocular surface and dry eye disease. The Committee created the ASCRS Preoperative OSD Algorithm.1
Preeya Gupta, MD, an author on the original paper and a member of the ASCRS Cornea Clinical Committee, said that the Committee is currently working on an update to the ASCRS Preoperative OSD Algorithm. Newer therapies for dry eye disease have been introduced. “We also want to focus on bringing education and awareness of this disease and its negative impact on outcomes in refractive cataract surgery,” she said.

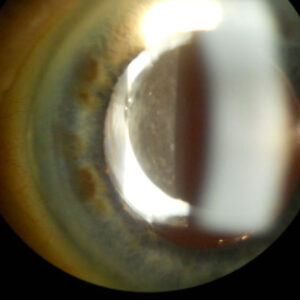
Source: Beeran Meghpara, MD
The Committee is currently drafting its updates, with a planned webinar on these updates early next year closer to publication.
EyeWorld has previously covered this topic and the ASCRS Preoperative OSD Algorithm and recently recapped presentations from a 2024 EyeWorld Corporate Education event in its Summer 2025 issue. One of these presentations from Christopher Starr, MD, gave an overview of the algorithm.
The ASCRS Preoperative OSD Algorithm functions as a flow chart to guide ophthalmologists through the testing, diagnostics, and treatment of visually significant OSD preoperatively. The goal was to create an algorithm that was consensus- and evidence-based, that could be integrated into the preoperative surgery visit, that had reliance on technicians and objective testing to reduce surgeon chair time, and that would identify all visually significant subtypes of OSD, not just dry eye disease, prior to surgery.
The algorithm involves a number of steps. The first step is to acquire the non-invasive refractive and biometric measurements, with the caveat that these tests might need to be repeated at a subsequent visit if visually significant (VS)-OSD is detected. For cataract surgery, these may include optical biometry, keratometry, tomography/topography, etc., and for laser vision correction, aberrometry, tomography, etc.
The second step is the OSD screening battery, with the goal of identifying all subtypes of OSD. This led to defining the term VS-OSD, or any OSD that can lead to IOL errors or refractive surprises, decreasing patient satisfaction and reducing visual quantity, quality, and performance postoperatively. It could also lead to a post-surgical infection like endophthalmitis and/or non-visually significant OSD that may worsen after surgery and become visually significant.
In assessing dry eye disease and OSD, physicians need to inquire about symptoms, however, signs are more important preoperatively (especially since many of these patients may be asymptomatic). To aid in symptom assessment, a new pre-surgical OSD questionnaire was created for the algorithm.
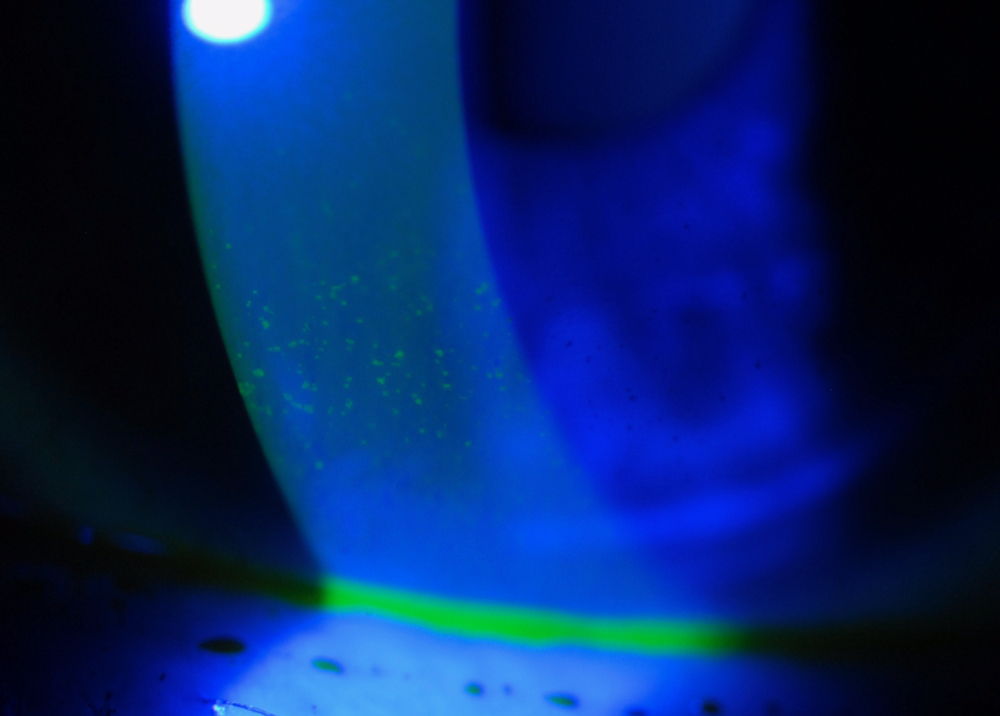
Source: Christopher Starr, MD
The algorithm also points to the importance of a slit lamp exam to assess the patient for VS-OSD. The LLPP technique—look, lift, pull, push—is critical in this step. It can also be important to test for corneal sensation and staining.
After assessing for OSD, the physician needs to determine if it’s visually significant and could potentially impact the surgical outcome. If VS-OSD is detected, it should be treated aggressively and ideally reversed before proceeding with surgery. Treatment options for VS-OSD are numerous, including prescription medications and procedural treatments.
Dr. Starr noted that the algorithm took multiple iterations and a few years to get it right.
In the 6 years since the paper was first published, there have been many advances in research, diagnostics, and treatments in the OSD and surgical spaces, Dr. Starr said, adding, “We thought that the time was right to update the algorithm and consensus recommendations.”
Dr. Gupta said the new paper will be in a similar format to the previous publication and will include an updated review of the literature. “We will dive into the algorithm, discuss prevalence and negative consequences of visually significant OSD, and review treatment strategies,” she said.
While Dr. Starr said it’s still a work in progress and far from being finalized, overall, the algorithm and questionnaire will be iteratively refined, and the paper will be updated to reflect the new knowledge and various FDA approvals since the first publication. “We will be highlighting the changes to the algorithm, questionnaire, consensus recommendations, and overall methodology,” he said. ASCRS Clinical Committee educational initiatives are largely driven by the annual ASCRS Clinical Survey responses, he said, adding that recent survey data showed that 15% of respondents think the prevalence of dry eye disease/OSD in their cataract patients is zero, and 18% would implant a multifocal or extended depth of focus IOL in a patient with preoperative OSD and “manage the OSD postoperatively.” “Clearly, we still have some educational work to do, and this is why we are updating the algorithm,” he said.
For those physicians just getting started with implementing the OSD algorithm into practice, Dr. Gupta stressed that “practice makes perfect.” “The beauty of this algorithm is that it is adaptable to whatever diagnostic tools you have in your clinic,” she said. “We think that anyone can screen for OSD in their perioperative patients, and simple diagnostic equipment and questionnaires can be used to find patients in need of treatment.”
“Our algorithm was designed to be easy to follow and easy to integrate into the pre-surgical evaluation, and many surgeons do follow it faithfully, partially, or have adapted their own version of it, and all of that is fine with us,” Dr. Starr said. “Our goal was to raise awareness on the importance of the ocular surface on surgical outcomes and to provide an easy framework for routinely managing these patients efficiently and successfully.”
About the physicians
Preeya K. Gupta, MD
Managing Director
Triangle Eye Consultants
Raleigh, North Carolina
Christopher Starr, MD
Director, Refractive Surgery
Director, Ophthalmic Education
Weill Cornell Medicine
New York Presbyterian Hospital
New York, New York
Reference
- Starr CE, et al. An algorithm for the preoperative diagnosis and treatment of ocular surface disorders. J Cataract Refract Surg. 2019;45:669–684.
Relevant disclosures
Gupta: Alcon, Azura, Bausch + Lomb, Harrow, Sight Sciences, Tarsus
Starr: AbbVie, Alcon, Aldeyra, Azura, NuVissa
Contact
Gupta: preeyakgupta@gmail.com
Starr: drstarr@gmail.com