Cataract
Winter 2025
by Ellen Stodola
Editorial Co-Director
When considering cataract surgery, one of the most basic steps is choosing the incision to be used. Several physicians discussed the impact of these incisions, sizing considerations, and important techniques and principles to ensure a successful surgery.
To take out a cataract, you have to make an incision, said Kevin M. Miller, MD. “Back in the old days, we didn’t make corneal incisions; we made scleral incisions because we didn’t have foldable lenses.” While modern-day corneal incisions come with the downside of needing to make a cut into the eye, a key benefit is they are small and can also help modify pre-existing corneal astigmatism. “We can use the architecture and placement of an incision to mitigate some of the eye’s astigmatism,” he said.
“I think it’s a very pertinent topic for surgeons to understand the impact of how your incision can impact the surgically induced astigmatism,” said Sumit “Sam” Garg, MD, noting a paper1 from Jack Holladay, MD, about induced astigmatism and the impact of incision location and size. “What he showed is that for most incisions placed at zero, meaning at the horizontal axis temporal, they have very little astigmatic effect with respect to the centroid error.” As a result, Dr. Garg said he places most of his incisions here. “I’m trying to be astigmatically neutral because in many of my patients, I’m treating astigmatism concomitantly,” he said. Factors like the width of the incision and the placement can impact the potential astigmatic effect of the incision. If you make the incision closer to the visual axis, you’ll have more of an astigmatic effect.

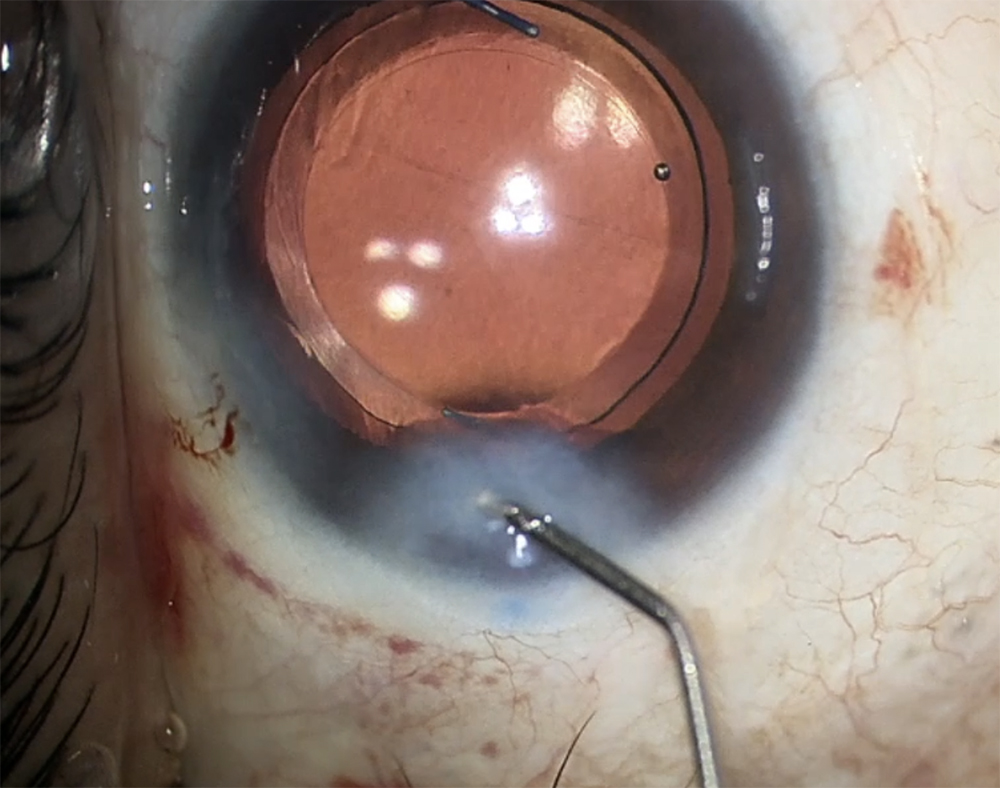

Source (all): Sumit “Sam” Garg, MD
Dr. Miller explained that the simplest incision is like a straight stab into the eye with a keratome blade. You can use this single-plane incision or a multi-plane incision. “The most common is a two-plane incision,” he said. “You make a groove, straight down at the limbus, and go inside the groove about halfway down to make the radial portion of the incision.” Using a femtosecond laser, multi-plane incisions can be done up to three planes.
He discussed incision types, noting the hinged incision concept from David Langerman, MD.2 It’s a two-plane incision where you make a deep cut for the groove that follows the limbus, then you go into the groove and make a second incision plane that goes radially toward the middle of the cornea and into the eye. “The groove is 450–500 microns deep, and the second radial incision is 1.75 or 2 mm in length,” Dr. Miller said. With this incision, there’s a triangular wedge of tissue on the inner aspect of the cornea with a hinge point that acts as a valve.
“If you raise the pressure in the eye, that little wedge of tissues slams against the hole and seals it off,” he said. “The higher the pressure in the eye, the better the incision seals.” In contrast, if you raise the pressure in an eye with a straight stab incision, the more you raise the pressure, the more it leaks, Dr. Miller said, adding that hinged incisions, if done properly, don’t leak nearly as much.
Dr. Miller also noted research from Paul Ernest, MD, on types of corneal incisions,3 comparing which sealed best. Dr. Ernest looked at square sclerocorneal incisions, square clear corneal incisions, and rectangular clear corneal incisions. “He found that square incisions in the cornea sealed best,” Dr. Miller said.
So, if you have a squared incision and hinge it, you’ll have a good corneal incision that seals well, Dr. Miller said. “If you place that incision appropriately, you can also reduce the astigmatism of the eye accordingly.”
Richard S. Hoffman, MD, chooses to make his cataract incision at the temporal location. “A small temporal clear corneal incision induces little if any astigmatism and will not cause long-term against-the-rule drift such as can occur with a superiorly placed incision,” he said. “Some surgeons will place their incision on the steep axis in order to help reduce cylinder, but I have found it more reliable to place the incision at 180 degrees and address astigmatism management with limbal relaxing incisions or toric IOLs.”
He also reiterated that most cataract incisions today are clear corneal. “The sclera can also be utilized in patients who have corneal pathology that might make a corneal incision problematic,” Dr. Hoffman said. The clear corneal incision can be made as a single planar entry or a two-plane incision made within a limbal grooved incision.
Dr. Hoffman noted that a single-plane incision is made with a diamond or metal keratome, starting just in front of the conjunctival insertion with the blade entering the anterior chamber with an upward direction parallel to the plane of the peripheral cornea.
The incision should have a similar length as the width to create a near square configuration, he said. Placing the incision in the depths of a 350- to 400-micron deep temporal grooved incision can help reduce small amounts of against-the-rule astigmatism that are too small for toric IOL placement, especially when paired with a second limbal relaxing incision 180 degrees away from the main incision.
Dr. Hoffman added that a scleral incision usually requires a conjunctival peritomy with or without the concomitant use of scleral cauterization. “A groove is usually created for the start of the scleral incision followed by dissection into clear cornea utilizing a diamond or metal crescent blade,” he said. “An alternative is a straight planar entry into the anterior chamber starting 1 mm posterior to the limbus and entering the anterior chamber at least 2 mm from the limbus. It is important to ensure that the entry site of scleral incisions into the anterior chamber is adequately anterior in order to avoid iris prolapse.”
Dr. Hoffman noted that scleral incisions are mainly utilized in patients with multiple radial keratotomy (RK) incisions. “Most individuals who have a conservative, eight-cut RK can still be approached with clear corneal incisions placed between the radial incisions,” he said, adding that when there are too many RK incisions to safely fit the cataract incision between the radial incisions, a scleral incision is necessary in order to prevent dehiscence of the RK incisions.
Every step in cataract surgery builds on the previous step. To have a good case, you have to start off with a well-constructed corneal incision.
Sumit “Sam” Garg, MD
“I personally utilize 1.1 mm bimanual incisions for my cataract surgery, placing the chopping infusion cannula through one incision and the bare phaco needle through the second incision,” he said. “With this configuration, the 1.1 mm clear corneal incisions can usually fit between a 24-cut RK.” He added that when it’s time to insert the IOL, a 2.2 mm scleral incision can be made, just posterior to the conjunctival insertion without creating a peritomy.
Most incisions are around 2.2–2.75 mm, depending on the blade you’re using and the sleeve, Dr. Garg said, adding that certain lenses require a little larger incision. “I tend to have a little larger incision because I like a high infusion sleeve with my phacoemulsification to allow for a very stable chamber,” he said.
Dr. Garg likes to use a biplanar or triplanar incision. He also noted that around 8–10 years ago, he started adopting a supraincisional pocket, known as a Wong pocket, above the phaco wound for routine patients. “I take my keratome, and about half a millimeter or so in front of the incision, I create a little pocket,” he said. “Behind that, I make my phaco incision, then I make a sideport incision. At the end of the case, I use the supraincisional pocket to hydrate the cornea.”
This, he said, is an easy pocket to hydrate, so you don’t have to worry about going into the sides of the incision and getting a lot of leakage as you hydrate the pocket. What you’re trying to do as you hydrate a corneal incision is plump it up so that it doesn’t leak. “You do that by pushing, with force, into the stroma of the cornea, injecting fluid, and getting it to balloon a bit,” Dr. Garg said. “With a Wong pocket, you hydrate in a similar fashion, but it pushes down on the incision, so it forces the incision closed. In my experience, it’s made my hydration step faster and more robust.” This technique was developed by Michael Wong, MD.
He noted that he will not use this pocket technique for certain patients, for example, in post-LASIK patients where he doesn’t want to create a cleft between the LASIK flap and underlying stroma. He also won’t use this option for patients where he knows he’s going to put in a suture, like those with RK or post-PKP.
“I’ve also incorporated the Wong pocket into my femtosecond laser template,” Dr. Garg said. “When I do my femtosecond laser, I do capsulotomy, fragmentation, and astigmatic incisions, then I’ll user the laser to create a precise pocket, and I’ll use a blade behind or underneath the pocket to make my main incision.”
Dr. Garg noted that there are some cases where he will choose to enlarge the incision beyond 2.75 mm, like if there is an unplanned vitrectomy and a lens needs to be placed in the sulcus. The injector can go through 2.75 mm, but he will make the incision closer to 3 mm to make sure he’s not placing too much pressure on the eye when trying to insert the injector, so he doesn’t promote vitreous prolapse.
Dr. Hoffman said that surgeons should be familiar with creation of both clear corneal and scleral incisions, and he added that practice in a wet lab using either pig eyes or human cadaver eyes is the best means for perfecting these incisions.
Dr. Garg said there are many textbooks that have been written on wound construction, noting the book Eye Surgery: An Introduction to Operative Techniques by Georg Eisner has illustrations on incisions and wounds. “It’s from 1990, but it’s a nice resource when it comes to any wound construction,” he said.
“We’ve come a long way with cataract surgery, but some of the principal features of cataract surgery and fundamentals have remained the same, and one of those is certainly wound construction,” Dr. Garg said. “I think understanding that will make you a better surgeon because knowing the different kinds of wounds you can make, the pros and cons of how they act, when you should use them, and how they close on their own is important. Every step in cataract surgery builds on the previous step. To have a good case, you have to start off with a well-constructed corneal incision.”
About the physicians
Sumit “Sam” Garg, MD
EyeWorld Chief Medical Editor
Vice Chair of Clinical Ophthalmology Medical Director
Professor of Cataract, Corneal, and Refractive Surgery
Gavin Herbert Eye Institute
University of California, Irvine
Irvine, California
Richard S. Hoffman, MD
Clinical Associate Professor of Ophthalmology
Casey Eye Institute
Oregon Health & Science University
Drs. Fine, Hoffman, & Sims
Eugene, Oregon
Kevin M. Miller, MD
Kolokotrones Chair in Ophthalmology
Chief of the Cataract and Refractive Surgery Division
Stein Eye Institute
David Geffen School of Medicine at UCLA
University of California, Los Angeles
Los Angeles, California
References
- Holladay JT, et al. Astigmatism analysis and reporting of surgically induced astigmatism and prediction error. J Cataract Refract Surg. 2022;48:799–812.
- Langerman DW. Architectural design of a self-sealing corneal tunnel, single-hinge incision. J Cataract Refract Surg. 1994;20:84–88.
- Ernest PH, et al. Relative strength of scleral corneal and clear corneal incisions constructed in cadaver eyes. J Cataract Refract Surg.1994;20:626–629.
Relevant disclosures
Garg: None
Hoffman: None
Miller: None
Contact
Garg: gargs@hs.uci.edu
Hoffman: rshoffman@finemd.com
Miller: kmiller@ucla.edu