Refractive: Opening doors
Winter 2025
by Ellen Stodola
Editorial Co-Director
While not a common approach or its primary indication, the ICL (STAAR Surgical) can be used as a supplementary/piggyback IOL in some patients. Drew Dickson, MD, Luke Rebenitsch, MD, and Carlos Rocha-de-Lossada, MD, PhD, FEBO, discussed how this off-label approach to using the ICL is opening doors to treat certain patients.
Dr. Dickson said the ICL as a piggyback lens is a unique scenario because it would require a big refractive miss.
For some people who are naturally nearsighted, sometimes the cataract surgeon might leave them fairly myopic, he said, adding that this doesn’t happen as much anymore. To use the ICL in this way, the patient needs to have the right prescription because the ICL’s lowest power is –3.
For example, Dr. Dickson said he had a patient recently who was left at around –5/–6 intentionally. You can consider ICL if they’re –2.5 or so. “That’s when I would first start thinking about it,” he said. “If there is a patient in that category, it’s the ultimate piggyback lens. If we’re planning to use a piggyback for patients now that’s not an ICL, it’s not as precise. There’s typically not an IOL calculation you do. It’s usually if they’re hyperopic or myopic, you take the prescription and have some fudge factor on what you think it should be. With the ICL, you’re still basing that just like you would with a normal ICL, so you’re taking the prescription and plugging measurements into the STAAR Surgical online calculator.” He said it’s also nice because it’s the only piggyback option with that sort of prescription where you can treat any astigmatism in the sulcus. “Up until recently, there was nothing even close,” Dr. Dickson said, adding that physicians can now also consider the Light Adjustable Lens (LAL, RxSight) in the sulcus for certain patients.
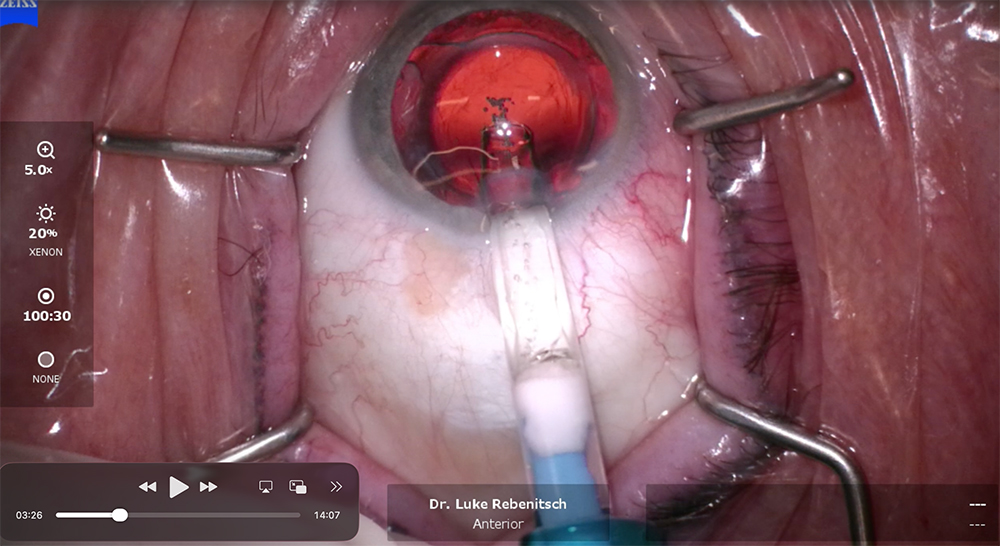
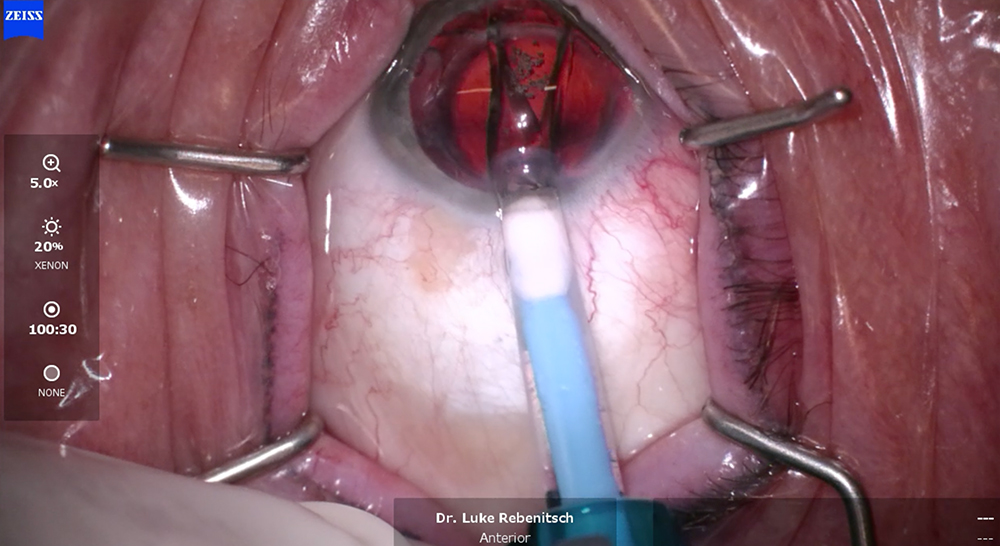
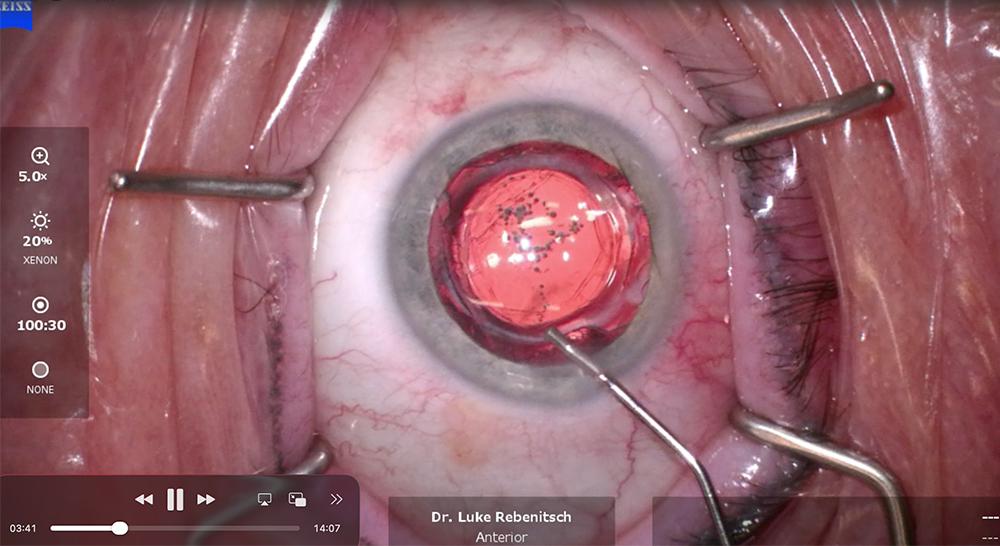
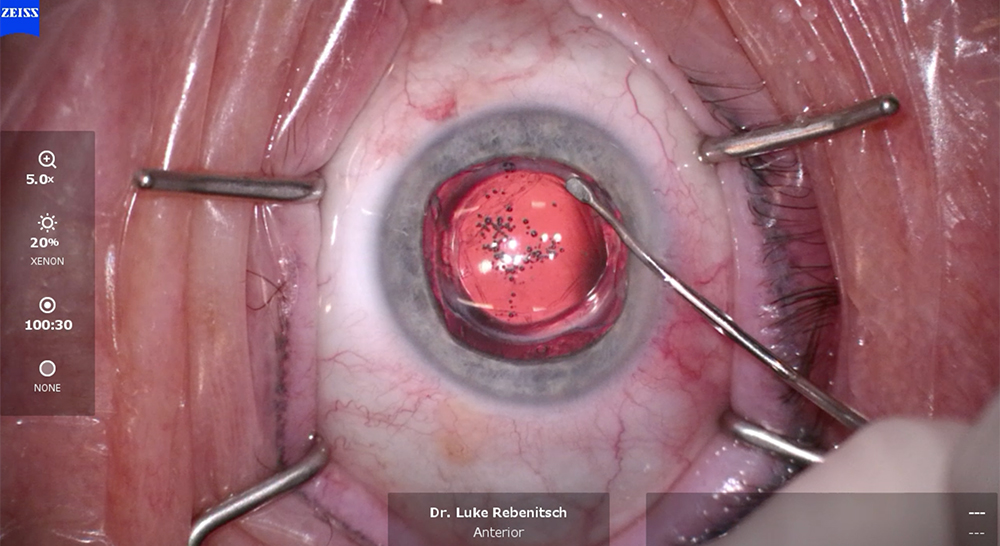
Source: Luke Rebenitsch, MD
Another benefit of the ICL is its removability. “Patients like the idea that it’s reversible or upgradeable over time,” he said. You don’t have to alter the natural anatomy of the cornea. Plus, Dr. Dickson said, it tends to have a high vision quality. “All those things that make us love the ICL in phakic patients apply to pseudophakic patients as well.”
Dr. Dickson said he’s used the ICL previously in patients with monofocal lenses, but it could be used in other cases, like with a trifocal.
Dr. Rebenitsch stressed that using the ICL in this manner is considered off label, but he’s used it this way a handful of times. He also noted that in the U.S., the ICL only goes down to –3, which is –2.5 at the spectacle plane. He agreed with Dr. Dickson that you’d have to really miss the target to use the ICL as a piggyback. “That being said, there’s some talk of having lower powered ICLs in the U.S.,” he said. “This could be used in the future potentially, even though it’s off label.”
Dr. Rebenitsch works in a 31-year-old cataract refractive practice, and he sees patients with previous RK and complex corneas. “Before the LAL, given that we see so many post-refractive patients, there were times when we just missed the target,” he said. “In those rare cases, I’ve used the ICL to hit the target, and it’s been effective. The chamber is typically already larger, so vault is a non-issue, and there’s no risk of inducing cataract. You do have to look at the angle and make sure it’s open enough to implant. But if anything, it’s easier to place in these cases than in a primary case.”
With a piggyback IOL, Dr. Rebenitsch said there can be a small risk of an interlenticular membrane, but with the ICL, there’s no lens-to-lens touch, so the risk of a membrane is zero. He added that there is also less risk of iris chafing or UGH syndrome with the ICL.
Dr. Rocha-de-Lossada said ICLs have become more common in refractive surgery, and based on the literature, the quality of the IOL materials, the visual acuity, refraction, and what the IOL produces in patients is very high. “Some authors started to think that if it was a good option in patients with a crystalline lens, why not use it in patients who have already had cataract surgery with some refractive error.”
Dr. Rocha-de-Lossada and colleagues have studied the usefulness of supplementary intraocular lenses.1 One study focused on the correction of presbyopia with supplementary IOLs and then to correct refractive error, focusing on astigmatism,2 he said. He and colleagues began to look at the ICL as an option. “It’s an interesting new option,” he said, adding that outcomes were very good. “We recently had the opportunity to review the literature on this topic and publish a scoping review highlighting the benefits of this new therapeutic option.”3
Some ophthalmologists might want to remove the IOL in the bag and put in a new IOL, but this comes with more risk, and he said that using a supplementary IOL is easier. The ICL as a supplementary IOL is reversible and easy to perform because it’s in the sulcus.
Other options for these patients include IOL exchange or laser vision correction. With an IOL exchange, if it’s an IOL that’s been there for a few years, or if they’ve had a YAG, if the capsule has contracted, etc., these exchanges could be harder to do, Dr. Dickson said. But if you can insert an ICL without messing with the IOL, that can be safer and quicker for patients. “You can still consider refractive enhancements like LASIK or PRK, but often if they’re getting these higher levels of prescription, it can be better to leave the cornea alone if you don’t have to mess with it,” he said.
Dr. Rebenitsch said piggyback is the least common enhancement option. Laser vision correction is the most common way to enhance. “An ICL would be used in patients with complex corneas where laser vision correction is not as precise.” He added that IOL exchange has its own risks. “For me, I tend to do piggybacks when there’s an open capsule and complex cornea,” he said. “IOL exchange is also fairly straightforward within the first year or two with a closed capsule, but once it’s open, the risk profile changes.”
Dr. Rebenitsch noted that using any piggyback IOL is considered off label. “As physicians, we can use any FDA-approved technology how we see fit.” That being said, he explains to patients that if he uses an ICL as a supplementary option, it is considered off label.
Dr. Rocha-de-Lossada noted that risks of using the ICL in this way are more or less the same as in indicated patients. There is a risk of infection and high intraocular pressure, but you have more space in the eye when you compare the size of the ICL to the normal crystalline lens. He said that so far the literature shows good results with low complications.
Dr. Dickson also said the same risks apply in these cases as with standard ICL surgery. He only considers this as an option in patients who had normal cataract surgery with the lens in the capsule. He noted that he wouldn’t choose to do a piggyback ICL if the lens were in the sulcus because the ICL sits in the sulcus. It’s important to ensure the patient has a healthy endothelium and that they don’t have glaucoma.
Since cataract surgery measurements are pretty accurate, Dr. Dickson said he only uses this technique on a couple of patients a year.
About the physicians
Drew Dickson, MD
Cataract and Refractive Surgeon
Kugler Vision
Omaha, Nebraska
Owner
Modern Vision Centers
West Des Moines, Iowa
Luke Rebenitsch, MD
Medical Director
ClearSight LASIK and Lens
Oklahoma City, Oklahoma, and Plano, Texas
Carlos Rocha-de-Lossada, MD, PhD, FEBO
Associate Professor
University of Seville
Head of the Ophthalmology Department
Vithas Málaga Hospital
Málaga, Spain
References
- Rocha-de-Lossada C, et al. Systematic review of the use of supplemental multifocal intraocular lenses in the ciliary sulcus for presbyopia correction. J Refract Surg. 2021;37:830–835.
- Rocha-de-Lossada C, et al. Supplemental toric intraocular lenses in the ciliary sulcus for correction of residual refractive astigmatism: a review. Ophthalmol Ther. 2023;12:1813–1826.
- Rocha-de-Lossada C, et al. Implantable collamer lens as an alternative supplementary intraocular lens to correct pseudophakic refractive error: a scoping review of the literature. J Refract Surg. 2025;41:e1254–e1261.
Relevant disclosures
Dickson: RxSight, STAAR Surgical
Rebenitsch: Bausch + Lomb, Johnson & Johnson, STAAR Surgical, Zeiss
Rocha-de-Lossada: Alcon, Bausch + Lomb, Medicontur, Oculus, SIFI, Zeiss
Contact
Dickson: ddickson@kuglervision.com
Rebenitsch: lrebenitsch@gmail.com
Rocha-de-Lossada: carlosrochadelossada5@gmail.com


