Cataract
Fall 2024
by Ellen Stodola
Editorial Co-Director
The IC-8 Apthera (Bausch + Lomb) was approved by the FDA in 2022. Since then, many physicians have incorporated it into their practice. With increased experience, some are discovering ways to apply this technology off label. Nicole Fram, MD, and Robert Ang, MD, discussed their experience using the lens, including ways that it can apply to patients who previously had limited options, particularly those with irregular astigmatism.
I say, ‘One eye gets better far vision, while in the second eye with the IC-8 Apthera, we will sacrifice some sharpness and brightness to gain intermediate and some near vision.’ If they are OK with this, we proceed.
Robert Ang, MD
The on-label indication is to put it in the non-dominant eye for extended depth of focus, Dr. Fram said. “They found the sweet spot in the FDA trial to be a target of –0.75 D, which typically achieves good uncorrected distance to 20/25 or 20/30 but also allows for the ability to read at intermediate,” she said. “The only caveat is there should be counseling about the dimming that can happen in low light. As you create a pinhole effect, you can see light and some contrast, but it’s mainly relevant in low light settings.”
Although Dr. Fram is using small aperture technology mainly in eyes with aberrated corneas, one can also use this technology for patients with regular corneas but who might need some extended depth of focus (EDOF) and are not a candidate for an EDOF IOL or a diffractive technology. “Another application for the IC-8 Apthera is in the circumstance where you’re not sure about the exact axis of the astigmatic correction and you need a forgiving technology,” she said.
Source: Robert Ang, MD
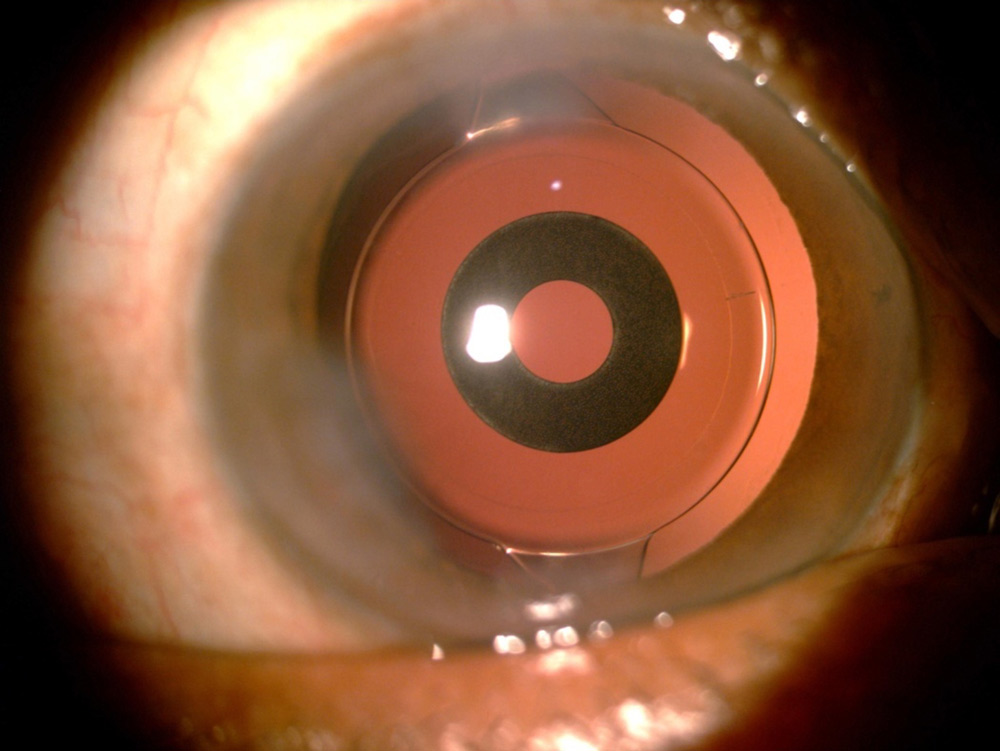
Dr. Ang, who practices in the Philippines, noted the approval in the U.S. for implantation in the non-dominant eye. The IC-8 Apthera has two unique features that occur simultaneously, he said. Small aperture optics can extend depth of focus and therefore can be used in presbyopia correction during cataract surgery similar to other EDOF IOLs. Secondly, small aperture optics filter out aberrations, especially from complex corneas, which distinguish it from any other IOL.
“Most of my colleagues who have used the IC-8 Apthera find its utility in managing post-refractive surgery eyes, such as previous RK, PRK, LASIK,” he said. “The aberration-filtering feature maintains or even improves distance corrected vision and quality of vision.” He added that the presbyopia capability is the bonus. Other presbyopia-correcting IOLs using diffractive, wavefront-shaping, or spherical aberration induction optics can worsen quality of vision and photic phenomena by inducing additional aberrations. “The IC-8 Apthera is my preferred lens choice for post-refractive eyes,” Dr. Ang said. “I have used this lens in clinical studies over 8 years and commercially for 1 year.”
Dr. Fram said that one of the exciting things about this concept is that the pinhole effect can also help patients with higher order aberrations (HOAs). “HOAs are the irregularities of the light rays as they hit the eye on whatever interface, and it got us thinking of some off-label use of this technology,” she said.
The idea would be if you create a pinhole effect, you can reduce the higher order aberrations, Dr. Fram said “We found that there’s this whole population of patients where we were saying, ‘You could get a PKP or DALK, wait a year, then do the cataract surgery and hope you don’t need a contact lens after for your best corrected vision, or we can do a monofocal lens and a scleral lens fitting.’ That was all we had to offer them, and many didn’t want to wear contacts.”
Source: Nicole Fram, MD
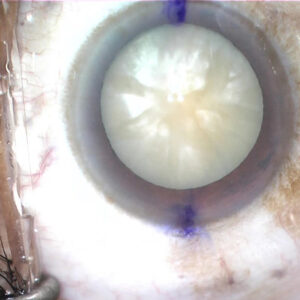
Dr. Fram and colleagues presented a paper on clinical outcomes in patients with irregular corneas receiving small aperture technology at the 2024 ASCRS Annual Meeting.1 The patients studied included those who had RK, keratoconus, post-PKP, and corneal scarring outside the visual axis.
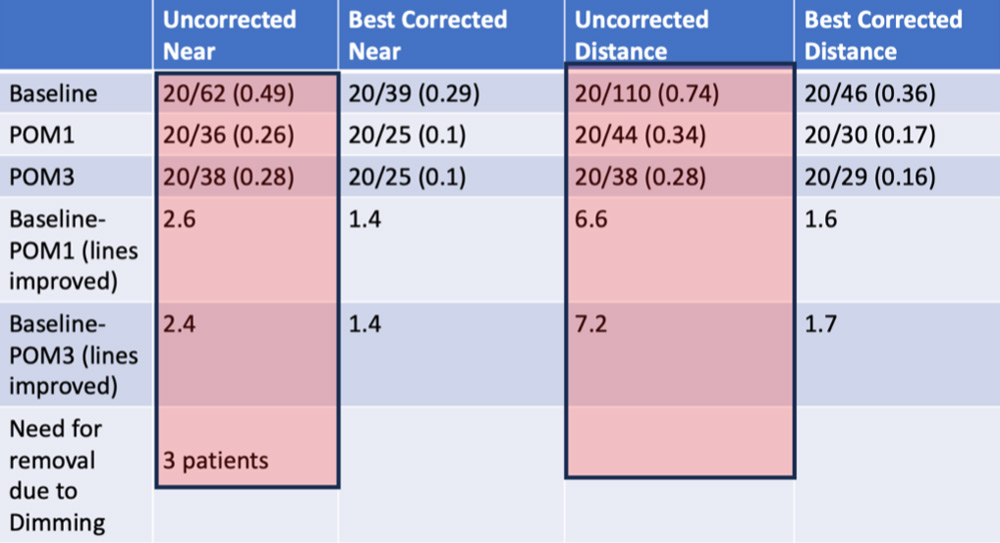
Fifty complex cornea eyes were examined, and Dr. Fram said the results were impressive with patients achieving 7.2 lines of improvement in uncorrected distance visual acuity and 2.4 lines of improvement in uncorrected near. However, all patients were counseled that they might need scleral contact lenses even after the IC-8 Apthera technology, she said.
Dr. Fram said a caveat with these patients is you need to ensure that there is no central scarring when you use the IC-8 Apthera technology. A preoperative pinhole test in the office or a pilocarpine 1% test is helpful to make sure that the dimming is acceptable to the patient.
The iTrace technology (Tracey Technologies) can simulate a small aperture, she added. That gives you a simulation when you remove HOAs of what the vision will potentially be, and it’s a good way to see if this would be the right technology for your patients. “If it’s too dim, then you know it’s not the right technology, and monofocal with scleral lens is the best approach,” she said.
“If the dominant eye qualifies for the IC-8 Apthera, and that’s the only lens that will correct the irregular cornea, I choose to do a bilateral approach,” Dr. Fram continued. If you leave the dominant eye with an IC-8 Apthera and the non-dominant eye with a monofocal, you run the risk of the patient noticing more of the dimming effect. Conversely, if the non-dominant eye has an IC-8 Apthera, you can use a regular monofocal in the dominant eye without issue.
Source: Nicole Fram, MD
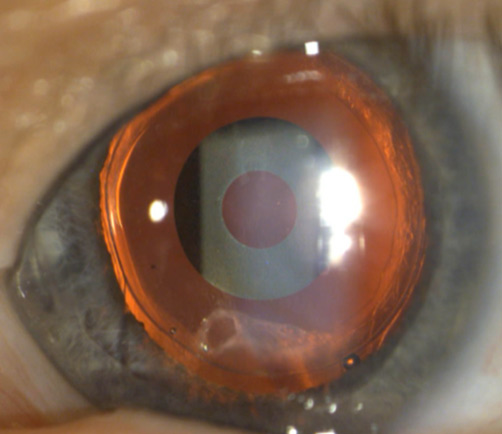
Dr. Fram said the “moral of the story” is that there have been some interesting developments in off-label applications of the IC-8 Apthera in a population that did not previously have a lot of hope or options. “We also are learning about the adaptation to the dimming through trial and error of who tolerates the dominant eye having this technology,” she said. It is important to counsel patients ahead of time there is a small chance you may have to remove it because of dimming. “With irregular corneas, you need to make sure the scarring is not in the central 1.6-mm zone, and if there is a chance the patient needs the small aperture in the dominant eye, consider off-label bilateral implantation. You want the pupil to dilate to at least 6.5 mm because you need to get around the inlay to do the YAG so you don’t hit the inlay inadvertently,” Dr. Fram said.
Dr. Ang also discussed some of the same off-label applications of this lens that Dr. Fram highlighted. Use of the IC-8 Apthera on complex corneas is becoming accepted because it improves the quality of vision of aberrated corneas, he said. The more aberrated cornea may not be the non-dominant eye, and in some instances, like bilateral RK eyes, both eyes will benefit from the IC-8 Apthera, so bilateral use can be acceptable.
In terms of counseling patients on this technology, Dr. Ang said he describes the drawbacks of this lens similar to monovision. “I say, ‘One eye gets better far vision, while in the eye with the IC-8 Apthera, you will sacrifice some sharpness and brightness to gain intermediate and some near vision.’ If they are OK with this, we proceed.” For targeting, Dr. Ang said the sweet spot of the lens is to achieve a mildly myopic outcome of MRSE –0.50 D to –1.00 D. “From my experience, these patients are the most satisfied,” he said. It’s also important to be sensitive to posterior capsular opacity. “If there is a grade 1 opacity within the aperture, and the patient notices a change in vision, whether distance or near, I proceed with YAG capsulotomy, which can be as early as 6 months postoperative,” he said.

Article Sidebar
Dagny Zhu, MD, Cataract Editorial Board member, shared how she has knocked down clinical and surgical challenges:
- Reverse optic capture can be useful for treating complaints about negative dysphotopsia post-premium IOL cataract surgery.
- Assembling preop dry eye kits for patients to purchase beforehand may decrease post-cataract dry eye complaints.
- YAG laser vitreolysis can effectively treat floater complaints post-cataract surgery. (For more on this, see “Floaters getting in the way of postop patient happiness?” on page 34.)
About the physicians
Robert Ang, MD
Asian Eye Institute
Makati City, Philippines
Nicole Fram, MD
Advanced Vision Care
Los Angeles, California
Reference
- Fram NR, et al. Clinical outcomes of the small aperture IOL for complex corneas with irregular astigmatism. Paper presented at the 2024 ASCRS Annual Meeting, April 5–8, 2024, Boston, Massachusetts.
Relevant disclosures
Ang: Bausch + Lomb
Fram: Bausch + Lomb
Contact
Ang: rtang@asianeyeinstitute.com
Fram: drfram@avceye.com