Refractive: Evolving
Winter 2024
by Liz Hillman
Editorial Co-Director

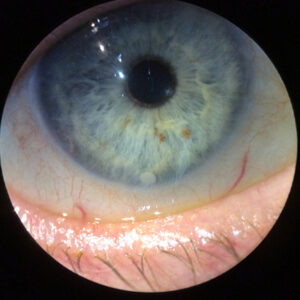
Source: Kenneth Beckman, MD
Crosslinking to stop progression of keratoconus and post-surgical ectasia has undergone an evolution both in the U.S., where it was first approved in 2016, and outside the U.S., where it has been in use significantly longer.
With new techniques in (or having recently completed) Phase 3 clinical trials to potentially move crosslinking to the next stage in the U.S., EyeWorld spoke with specialists to take a look back at where keratoconus monitoring and treatment was, where it is now, and what could be coming in the future.
Then: transplants
Prior to crosslinking becoming available in the U.S., there was no treatment for keratoconus patients until they needed corneal transplants.
“Documenting progression was important back then but for different reasons. Back in the day, there was nothing in the U.S. approved to stop progression,” said Kenneth Beckman, MD. “There were things to give you better vision in the moment, such as intrastromal cornea rings. Prior to crosslinking, patients basically lived with glasses and contacts until they needed a transplant. For as long as you could keep them functioning in a contact, you didn’t do the transplant. … That was the previous strategy.”
The tools to diagnose and monitor were not as sophisticated as they are now. Dr. Beckman said all that was available was topography (which was not as good as today’s technology), clinical signs (such as thinning or the Munson’s sign), or significant refractive changes.
Roy Rubinfeld, MD, said keratoconus management was “pretty primitive” back then. “You would hope they wouldn’t get worse, and hope is not a medical plan,” he said.
Now: epithelium off
In 2016, the FDA approved the Avedro crosslinking system—a combination of riboflavin loading on the cornea from which the epithelium had been removed followed by continuous UV light exposure for 30 minutes—for treatment of documented progressive keratoconus. Glaukos acquired Avedro in 2019. iLink—Photrexa Viscous (riboflavin 5’-phosphate in 20% dextran ophthalmic solution) and Photrexa (riboflavin 5’-phosphate ophthalmic solution) for use with the KXL System—remains the only FDA-approved crosslinking system in the U.S.
Since this became available, alongside significantly improved diagnostics, many changes have occurred in keratoconus management. New corneal imaging systems (topography and tomography), Dr. Beckman said, have allowed earlier and more accurate diagnosis of keratoconus, which is important to identify and treat early to stop progression and prevent subsequent, irreversible vision loss. Dr. Beckman also said epithelial mapping has been helpful in differentiating thickened epithelium from a steep cornea.

Source: William Trattler, MD
Tracking progression of keratoconus has now become critical, as documented progression is indicated for use with the currently approved crosslinking system. Dr. Beckman said it’s also important to consider risk for progression. If you’re seeing a young patient who already has a significant cone, waiting to document progression could result in increased vision loss that could be prevented. He said these cases will often make it through insurance approval with an appeal.
William Trattler, MD, said one of the major hurdles that came about after FDA approval of crosslinking was a change in mindset. Referring optometrists and comprehensive ophthalmologists had to be educated on careful monitoring of keratoconus and quick referrals for crosslinking. “Our goal has always been to diagnose early to identify patients because if we treat them early we can prevent more significant vision loss,” Dr. Trattler said. “If they are more advanced, we can still treat them so they don’t get hydrops or more serious complications and need a transplant. It’s really been a tremendous technology shift, and I think … the sooner that we can catch patients, the sooner we can treat them, the less morbidity will occur.”
In addition, Dr. Trattler said that understanding of who can/should be crosslinked has evolved. “Patients with thin corneas and steep corneas can achieve successful strengthening of their corneas with crosslinking. In the past, there were some theoretical worries about corneas being too thin to undergo crosslinking, but studies have demonstrated that the patients with very thin corneas (even under 300 microns) can safely undergo crosslinking. For example, the sub400 protocol by Farhad Hafezi, MD, has demonstrated that reducing the time for UV light exposure can safely and effectively allow for crosslinking to be performed in corneas in the 200 to 400 micron range,1” he said.
Dr. Rubinfeld added that patients over 30, 40, 50, and even 60 can rapidly progress despite information in old textbooks. He emphasized the need for continued monitoring even into older age.
Next up: transepithelial
In the U.S., transepithelial crosslinking protocols are in clinical trials.
“Doctors have been interested in FDA-approved transepithelial crosslinking for a long time because it has the potential to be a faster procedure that may be more comfortable for patients,” said Brandon Ayres, MD, who was involved in Glaukos’ trials. “Without the need for epithelial removal, we might expect more rapid post-treatment healing and visual recovery and a reduction in the already low risk of complications from a less invasive procedure. However, we don’t want these benefits to come at the cost of efficacy of the procedure, so I think we all have been awaiting the results of ongoing clinical trials with both caution and optimism.”
Source: Roy Rubinfeld, MD
In October 2024, Glaukos reported positive topline results from its second, confirmatory Phase 3 pivotal trial for Epioxa, a system that uses a novel riboflavin formulation, a pulsed, higher-intensity UV-A irradiation protocol, and supplemental oxygen. This trial enrolled 312 eyes. According to the company’s press release announcing topline results, Epioxa achieved its primary efficacy outcome, “demonstrating a Kmax treatment effect of –1.0 D determined as prospectively defined least square mean Kmax change from baseline in the Epioxa treated arm versus the sham/placebo-controlled arm at the month 12 study endpoint.” A New Drug Application is expected to be submitted to the FDA by the end of 2024.
In its first Phase 3 clinical trial for Epioxa, the treatment resulted in a statistically significant 1 D or greater difference in Kmax from baseline to 6 months compared to the control group, demonstrating the ability to stop or reduce keratoconus progression.
Epion Therapeutics completed a Phase 2 clinical trial, which enrolled 2,258 participants with corneal ectasia, for its EpiSmart system in 2021 and began a Phase 3 clinical trial in October 2023. Michael W. Belin, MD, Chief Medical Officer for Epion Therapeutics, said recruitment for the Phase 3 trials should be complete by the end of 2024/early 2025. The EpiSmart, Phase 3 trials, instead of using Kmax as a metric, which Dr. Rubinfeld said is not correlated with vision, uses visual acuity as its efficacy metric. The two concurrent Phase 3 trials will enroll 800 subjects at 20 investigational sites in the U.S., with patients receiving bilateral, simultaneous treatment when indicated, according to the company’s press release.
Dr. Belin said the EpiSmart system is unique in riboflavin concentration (“up to 5x more concentrated” than some other systems), its proprietary riboflavin loading sponge, which provides constant contact of the drug to the corneal surface, and with the addition of sodium iodine, which he said enhances penetration of the drug through the epithelium.
“It stabilizes the riboflavin once it gets into the stroma so we don’t drop during the UV application and …. [contributes] oxygen back into the cycle,” Dr. Belin said, adding later, “the other thing that I think is unique about our protocol … is that we have the ability to treat both eyes simultaneously if both eyes qualify for entrance into the study.”
Dr. Rubinfeld, one of the physicians at the forefront of the epithelium-on crosslinking technology, said having a crosslinking system in the U.S. that can be performed upon initial diagnosis of keratoconus (not needing to wait for documented progression) and in a transepithelial manner will greatly benefit patients. Dr. Beckman agreed, though he said, for now, the approved epithelium-off procedure remains the gold standard, and he would perform it on his own child, if he needed it.
“Once epi-on is approved, if it is even close to epi-off, no one will be doing epi-off, they’ll be doing full-time epi-on,” he said, noting that this would likely be due to a more favorable risk-benefit profile. “I think it will be first line because of safety, but that doesn’t mean it’s better. … If your goal is stopping progression, and epi-off gives you a diopter of flattening and epi-on gives you a third of a diopter of flattening, both of them have stopped progression, but you might say the risk is so much less with epi-on, I’d much rather do that. I do think it’s the way of the future, and I do think that once it’s there it will be everyone’s first line, … assuming you’re allowed and have the access.”
Dr. Belin said a transepithelial procedure will likely have a better risk-benefit ratio, allowing physicians to intervene at the earliest possible stages.
“I think that will ultimately be the benefit of epithelium-on crosslinking, allowing us to not wait until there is permanent loss of vision but to intervene in patients with true disease at the earliest point of diagnosis,” Dr. Belin said.
Dr. Trattler said a transepithelial procedure could provide a better patient experience because there is no epithelial defect and lead to quicker visual recovery, but he also said these procedures are looking to increase efficacy as well through pulsed light and other methods to increase oxygen availability.
“Pulsing of UV light (as compared to continuous UV light), in our experience, has worked well to strengthen the cornea. … You’re achieving a stronger effect when the three critical components to the crosslinking reaction are present: riboflavin, UV light, and oxygen. When the UV light is on, the oxygen in the cornea depletes, so techniques that allow for increased oxygen availability in the cornea can help provide a more efficient crosslinking reaction. Both the Glaukos and Epion Therapeutics clinical trials for epithelial-on crosslinking use pulsed UV light to increase oxygen availability. Glaukos also has an eye mask that delivers additional oxygen to the corneal surface. With more oxygen, the crosslinking reaction is more effective,” Dr. Trattler said.
About the physicians
Brandon Ayres, MD
Cornea Service
Wills Eye Hospital
Philadelphia, Pennsylvania
Kenneth Beckman, MD
Director of Corneal Surgery
Comprehensive Eyecare of Central Ohio
Westerville, Ohio
Michael W. Belin, MD
Professor of Ophthalmology and Vision Science
University of Arizona College of Medicine
Chief Medical Officer
Epion Therapeutics
Tucson, Arizona
Roy Rubinfeld, MD
Clinical Professor
Georgetown University
Medical Center
Medical Director, ReVision
Washington, D.C., and Rockville, Maryland
William Trattler, MD
Director of Cornea
Center for Excellence in Eye Care
Miami, Florida
Reference
- Hafezi F, et al. Individualized corneal cross-linking with riboflavin and UV-A in ultrathin corneas: the sub400 protocol. Am J Ophthalmol. 2021;224:133–142.
Relevant disclosures
Ayres: Glaukos
Beckman: Glaukos
Belin: Epion Therapeutics
Rubinfeld: Epion Therapeutics, www.CXLUSA.com
Trattler: Epion Therapeutics, Glaukos
Contact
Ayres: bayres@willseye.org
Beckman: kenbeckman22@aol.com
Belin: mwbelin@epiontx.com
Rubinfeld: rsrubinfeld@gmail.com
Trattler: wtrattler@gmail.com