Refractive
September 2023
by Ellen Stodola
Editorial Co-Director
The IC-8 Apthera IOL (Bausch + Lomb) is now available in the U.S., and several surgeons shared how this technology fits into their practice and for which patients. Arthur Cummings, MD, also provided an international perspective.
Shamik Bafna, MD, who was involved in the FDA clinical trial, said that this lens works well in any patient who has an irregular cornea, especially irregular astigmatism like that seen in keratoconus. However, in the clinical trial, the lens was not used in patients with irregular corneas.


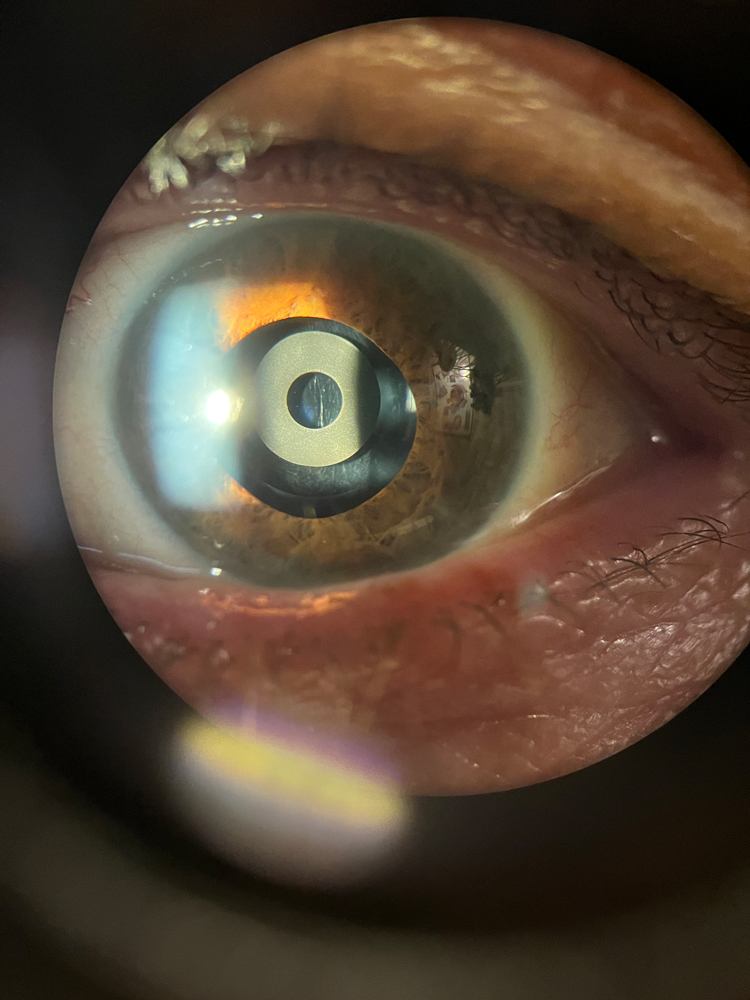
Source (all): Arthur Cummings, MD
In these cases, the cornea is limiting the quality of vision. A toric lens can correct regular, symmetrical astigmatism, “but in an irregular cornea, we don’t have a custom toric lens where it has less astigmatism correction on one side and more on the other. In the past, prior to approval of the IC-8 Apthera, we would attempt to use a toric lens in these [cases], and it would be hit or miss,” he said. “The other factor is if someone was used to wearing a gas permeable contact lens, we would not use a toric contact lens because it would make fitting of the gas permeable contact lens more challenging.” The IC-8 Apthera works well for patients who have an irregular cornea because it has a filter that blocks all of the peripheral light rays, so it only allows the central light rays to come through. In a cornea that has irregularity, it’s hard to focus with all of the light rays peripherally, so this allows the central light rays that don’t have irregularity to focus directly on the retina.
“If someone has keratoconus, if you put in the IC-8 Apthera lens that has a filter, we’re only allowing the clean, central light rays to go through,” he said. “This is the most common case in which it’s used, but it’s something we’re using off label because we know from our colleagues in Europe that it works well in this situation.”
The lens has been FDA approved to correct astigmatism up to 1.5 D, which Dr. Bafna said helps to correct a range of vision by using small aperture optics. He likened it to an EDOF lens, more so than a multifocal that splits light. It increases the overall depth of field and increases the overall range of focus, he said. Extended range of focus is what the IC-8 Apthera is currently FDA approved for, placed in the non-dominant eye.


Source (all): Arthur Cummings, MD
While keratoconus is the most common reason for using this lens off label for irregular astigmatism, Dr. Bafna said things like Salzmann’s nodules and pellucid marginal degeneration can create an irregular amount of astigmatism. Patients with prior RK are also likely to have some irregularity in their cornea. “What’s hard with RK is there’s a lot more variability in terms of the final visual outcome; there’s a lot more variability in our calculations,” Dr. Bafna said, adding that these patients may also have diurnal fluctuations.
There are some patients who may not be ideal candidates for this lens. Dr. Bafna noted that due to the filter in the lens, most patients will get 30–40% less light coming into their eye. If you use it unilaterally, it’s important to let patients know that they will notice that there’s less light and things will appear dimmer in that eye.
“A lot of our patients have monovision prior to cataract surgery,” he said, “but before cataract surgery, the natural lens gives them a bit of additional range of vision. One technique often used to simulate monovision is to put a monofocal lens in both eyes.”
Source: Blake Williamson, MD
The whole concept is range of vision, Dr. Bafna said. “A monofocal at near will be good at a particular point, but if you move your hand in and out, it gets out of focus. What’s nice about this lens is I can target –1 or –1.25, so I can give patients that entire range of vision.”
Karl Stonecipher, MD, said he has been familiar with this lens for some time. “On label, we’re looking at those patients who are a good monovision fit,” he said. “For me, they have less than 2 D of cylinder because the lens neutralizes 1.5 D. … I think for that classic depth perception monovision patient who wants great distance, it’s a fantastic lens.”
In patients who have a highly aberrated cornea—whether RK, hexagonal RK, LASIK with decentration, PRK with higher order aberrations and small optical zones, or keratoconus—Blake Williamson, MD, said these patients do exceptionally well with the lens. He will usually start with the most aberrated eye first to see how the patient does. Dr. Williamson noted that he’s generally using the IC-8 Apthera for off-label indications. If you ask most refractive surgeons, if the patient has a healthy cornea and desires presbyopia correction, the surgeon is most likely going to use an EDOF/multifocal/trifocal IOL, he said. The area where there’s been a need is in the post-RK, keratoconic, and post-LASIK space. While the Light Adjustable Lens (LAL, RxSight) is available, Dr. Williamson said this can be a heavy lift for some surgeons and patients in terms of the capital expense, the number of visits required to lock in refraction, and the need to wear glasses in between treatments. “The thought is that we have another device we can use without having to spend any money on a machine, and it fits better into the workflow for those difficult to treat eyes,” he said.
Dr. Williamson has been combining the IC-8 Apthera in the non-dominant and the LAL in the dominant eye. “To me that’s a wonderful opportunity for someone who has a cornea that’s severely aberrated because of keratoconus or RK,” he said, noting that surgeons using the IC-8 Apthera internationally are generally only using it bilaterally in extreme cases.
“I think it’s got an array of options available in the big picture. I find patients in whom I thought they would need something additional, and it’s amazing how the pinhole effect makes a difference.”
Karl Stonecipher, MD
There is the possibility of dimming, but Dr. Williamson said that this may be a small sacrifice for good functioning vision in both eyes. “If you have someone not doing a lot of nighttime driving, usually they’re willing to give that up. It’s not dissimilar to having the halo/glare/starburst talk with multifocal/EDOF patients,” he said. “The vast majority are more than happy to deal with that to have the gain that they do have. I think that bilateral IC-8 Apthera is going to be more common for those eyes.”
“If you do an LAL in the first eye, you know what their reading is going to be like, and if you think they’re not a monovision candidate, I might not put an LAL in second eye. I would do IC-8 Apthera on label,” Dr. Stonecipher said. He added that if you have a patient in whom you’re uncertain if monovision will work, and they haven’t had it before, an LAL would be a benefit, and it helps the patient know what they’re getting when choosing for the second eye.
Dr. Williamson said that one thing that has surprised him is the lens only goes down to 10 D. For extreme myopes, particularly those with keratoconus, there might not be a lens power for that. However, Dr. Williamson noted that he did a case where he was anticipating a myopic surprise and was very straightforward with the patient about this. However, the patient came back 20/15 J2 several days postop with the IC-8 Apthera. “Sometimes that pinhole can gobble up a lot of refractive error, not just coma and astigmatism, but even sphere,” he said.
Dr. Cummings has about 8 years of experience with the IC-8 Apthera. He said he mostly uses it when patients are dissatisfied with their quality of vision. “If someone had previous corneal refractive surgery and immediately after experienced glare and halos, it is likely from corneal origin,” he said. “If they did well initially and only became symptomatic once the cataract was diagnosed, the visual symptoms are likely from the cataract. Devices like the iTrace [Tracey Technologies] are useful for both patients and surgeons, making complicated optics understandable and showing both parties where the main issue lies. Is the greatest source of higher order aberrations external (cornea and tear film) or internal (lens and vitreous)? Address the source of greatest error first and explain to the patient that the vision will not be perfect until both have been addressed.” In the case where further corneal surgery is either impossible or unwanted, using the IC-8 Apthera can improve the overall wavefront from internal and external sources, Dr. Cummings said.
Dr. Cummings did note that someone with a perfect cornea might consider less light with the IC-8 Apthera to be an issue if they have not seen a significant reduction in glare and halos because there were no corneal higher order aberrations to start with. “The IC-8 Apthera works well in cases with corneal aberrations, including keratoconus, post-RK, post-decentered corneal ablations, or cases with irregular astigmatism,” he said. “I have also found that patients with amblyopia often gain more vision than I would have expected, perhaps due to addressing the ‘crowding effect’ with the small aperture IOL.”
Technique considerations
Dr. Bafna said part of the approval process for surgeons who want to use this lens is they’re required to read about how to do a YAG because it’s a little different for this lens. The company asks you to YAG in a specific manner in these cases. “If you do it the normal way, patients will have floaters after the YAG,” he said. “In these patients, because they’re looking through this small, 1.6 mm aperture, if there are any floaters in the middle, it’s going to have a bigger impact on the patient’s overall vision.”
Dr. Cummings also said it’s important to be very particular with the YAG laser, avoiding laser pulses in the center of the mask. “It is advised to laser outside of the mask with the hinge inferiorly, and after the YAG laser capsulotomy, ideally the posterior capsule will flop posteriorly and hang inferiorly out of the pathway of the incoming light beams,” he said. “On occasion, this won’t go entirely according to plan, then you must do the YAG through the aperture in the center of the mask to detach the posterior capsule from the IOL surface. A small nick in the IOL is more symptomatic here, so it is important to take extra care.” He also said to determine your surgically induced astigmatism with this IOL, as the incision size is bigger than usual at 2.7 mm, and sometimes even larger. The IOL performs well if the final astigmatism is <1.5 D, so it is often prudent to do the surgery on axis to reduce the astigmatism.
In terms of technique and implantation of the lens, Dr. Bafna said the process is straightforward. There is an injector approved for use with the lens. He also mentioned the larger incision that might be needed with the IC-8 Apthera to avoid too tight of a fold that could damage the filter.
Dr. Williamson said he often uses a 2.5-mm incision during surgery but uses a larger one for the IC-8 Apthera. “What a lot of people won’t appreciate is it has to go through a 3-mm incision,” he said. “If I’m doing an on-label patient, I will typically use a 3-mm blade, larger sleeve, and surgery is the same. You just don’t want to try to use a 2.4-mm sleeve in a 3-mm wound. It leaks and makes the surgery that much harder.”
Future advances
In terms of future developments, Dr. Cummings said he would like to have a pre-loaded version of the IOL and a toric version. Often these aberrated corneas have significant amounts of astigmatism, he said.
Dr. Bafna said he’d be interested in seeing different aperture sizes for the lens in the future. Right now, it’s one size fits all, but depending on the individual and based on what their pupil size is and how much irregularity they have in the cornea, he would want the surgeon to have options to choose lenses with different size openings. However, he noted that the current opening works well for the majority of patients.
Dr. Stonecipher stressed that the IC-8 Apthera is another great tool in the toolbox, and he doesn’t want to pigeonhole it in the complex corneas. “I think it’s got an array of options available in the big picture. I find patients in whom I thought they would need something additional, and it’s amazing how the pinhole effect makes a difference,” he said.
About the physicians
Shamik Bafna, MD
Cleveland Eye Clinic
Brecksville, Ohio
Arthur Cummings, MD
Medical Director
Wellington Eye Clinic
Dublin, Ireland
Karl Stonecipher, MD
Clinical Professor of Ophthalmology
University of North Carolina
Clinical Adjunct Professor of Ophthalmology
Tulane University
Greensboro, North Carolina
Blake Williamson, MD
Williamson Eye Center
Baton Rouge, Louisiana
Relevant disclosures
Bafna: Bausch + Lomb
Cummings: Alcon, Bynocs, NanoDrops, REVAI, Scope, TearLab, Vivior
Stonecipher: Alcon, Bausch + Lomb, Johnson & Johnson Vision, Rayner
Williamson: Bausch + Lomb
Contact
Bafna: sbafna@midwestvision.com
Cummings: abc@wellingtoneyeclinic.com
Stonecipher: stonenc@gmail.com
Williamson: blakewilliamson@weceye.com