Cataract: Complicated cases
September 2023
by Liz Hillman
Editorial Co-Director
In the years since Shin Yamane, MD, PhD, presented on flanged double-needle intrascleral haptic fixation (2017),1 many surgeons have adopted the technique, but it’s not without complications that require preparation and management.
“There are many potential complications from intrascleral haptic fixation techniques, such as the Yamane technique. Herein we discuss some of the most relevant and worst,” Austin Nakatsuka, MD, and Jeff Pettey, MD, wrote in an email to EyeWorld.

D. Brian Kim, MD, also weighed in on the topic. A literature search, he said, failed to reveal exact incidence of complications with this technique, but “it’s safe to say the incidence is higher while on the learning curve, and it tends to be steep,” he added.
“These technical challenges have led surgeons to develop various adaptations, such as using a trocar instead of needles while others externalize the right side needle outside of the main incision to more easily cannulate the more challenging trailing haptic,” Dr. Kim said. “It’s difficult to assess frequency of complications when there are so many variations. With my own modifications, I have been fortunate to reduce the frequency and avoid catastrophic complications thus far, and currently, I do not tend to struggle with problems related to the technique.”
Dr. Kim, Dr. Pettey, and Dr. Nakatsuka provided their thoughts on some of the more common complications that can occur with intrascleral haptic fixation as well as pearls for handling each situation.
Choroidal hemorrhage: When passing needles through the sclera, Dr. Nakatsuka said the needles may intersect blood vessels and cause bleeding, which can be more significant in older individuals on anticoagulation medications but can also happen in younger individuals. See Figure 1 for an example.
“In our experience, this happens in roughly 1–5% of cases,” he wrote. “Depending on the severity of the bleeding, it may be treated medically with topical and/or oral steroids and cycloplegics versus surgical drainage.”
Dr. Pettey and Dr. Nakatsuka’s pearl for this situation was to stop anticoagulant use, if possible, in high-risk patients and to cauterize scleral vessels if needed.
Uveitis-glaucoma-hyphema (UGH) syndrome: “After placement of the lens, the optic or haptics can come in contact with the posterior face of the iris, leading to the dreaded trifecta of UGH,” Dr. Pettey said. “Ironically, the Yamane technique is sometimes used as a surgical treatment for UGH caused by previously implanted IOLs,” Dr. Nakatsuka added. “Still, it can cause UGH in its own right and most often requires a revision to address the negative sequela.”
To avoid UGH, Dr. Pettey and Dr. Nakatsuka said to ensure the lens is centered without tilt after viscoelastic removal. “Always place at least one iridotomy, and consider placing haptics further from the limbus (e.g., 2.5–3 mm instead of 2 mm), especially in cases where the iris is highly mobile and floppy. Although controversial, one can consider shortening the haptics,” Dr. Nakatsuka wrote.
Dr. Kim also said that if the needles are pierced through the sclera too anteriorly, it could cause the haptics to rub the overlying uveal tissue resulting in UGH or CME.
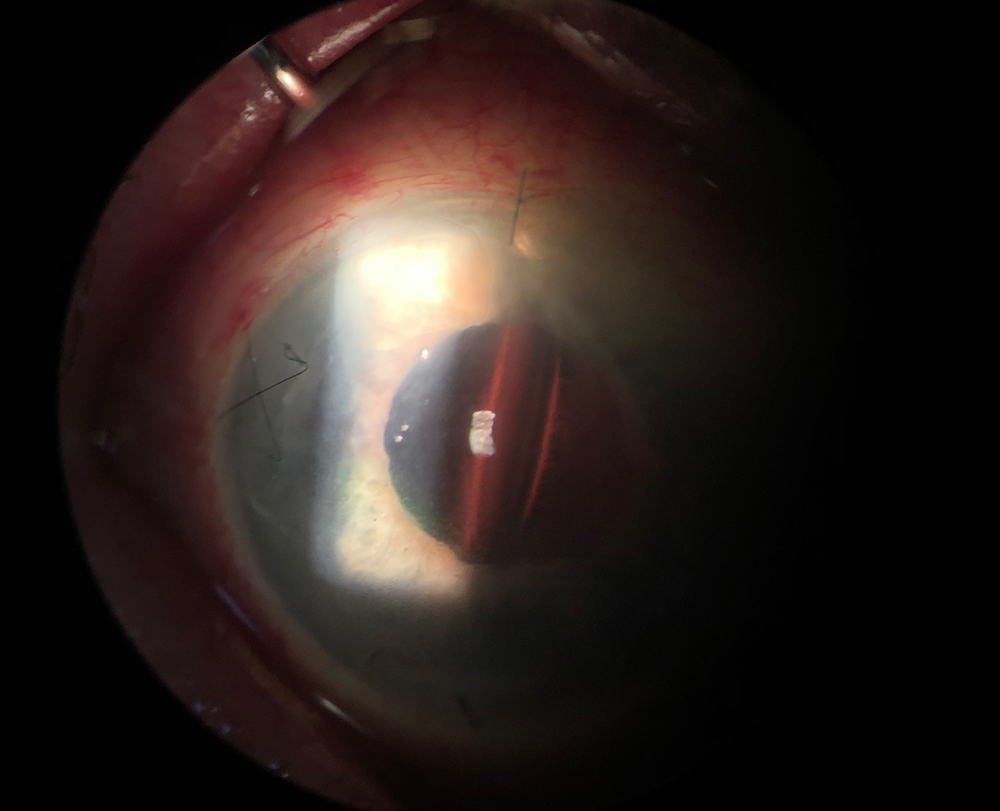
IOL decentration or tilt: This complication can occur due to asymmetrical scleral tunnels at different lengths or angles, Dr. Pettey and Dr. Nakatsuka said. To ensure proper centration, Dr. Pettey and Dr. Nakatsuka advised “meticulous pre-surgical marking with calipers and a Mendez ring to ensure targets are precisely 180 degrees apart, and mark the center of the cornea. Close observation of the scleral indentation during the docking procedure can alert the surgeon to an asymmetry between each side to ensure symmetric tunnels. Ensure that the globe is firm during the scleral needle insertion and avoid hypotony throughout the procedure. We recommend maximal pupil dilation to facilitate visualization during the docking step.” (See Figure 2).
Dr. Nakatsuka experienced a few cases of rotation of the haptic at the optic-haptic junction with the CT LUCIA lens (Carl Zeiss Meditec), although it appears to be isolated to a particular batch of these lenses. Dr. Kim also mentioned the recent issues observed with the CT LUCIA lenses, which he described as a “rotisserie rotation.” “Surgeons have observed that these haptics are not completely fused within the optic, causing them to rotate,” he said. “There is a technique called laser-lock,2 which uses the endolaser to essentially melt the haptic to the optic to address this.”
Lens/optic capture: Dr. Nakatsuka has experienced a few cases where the lens optic moves in front of the iris pupil. Floppy iris appears to be a risk factor for this complication (see Figure 3).
In addition to similar pearls for avoiding UGH, Dr. Pettey and Dr. Nakatsuka said that treatment options include miotics, supine positioning with miotics, laser iridoplasty, or surgical pupilloplasty to prevent the lens from coming forward. They said some surgeons recommend multiple peripheral iridotomies but noted the efficacy is still unclear.
Dr. Yamane recommends a 7.0-mm optic X-70 IOL (Santen) to avoid pupillary capture of the optic, but Dr. Kim said optic capture can still occur if the IOL is too close to the iris plane.
“Rather than placing the needles 2 mm posterior to the limbus, I prefer to place them further back at 2.5 mm and target –0.50 D for a plano refractive result,” he said. “With this modification, along with always placing a temporal surgical peripheral iridectomy to avoid reverse pupillary block, I have not experienced any cases of optic capture.”
Flagpole sign: Dr. Kim said that there needs to be adequate scleral support for the haptics with this technique. “If there is inadequate scleral support for the haptics because the needles are not tunneled through the sclera, the haptics may point up in a more vertical orientation, which I’ve coined the ‘flagpole sign,’” he said. “If there is a flagpole sign, this means the optic is sagging posteriorly within the vitreous space, which would induce optic tilt and astigmatism. A self-check to know the IOL is placed correctly is when you observe the haptics are lying flat to the sclera when the needles are pulled out.”
Hypotony: Dr. Pettey and Dr. Nakatsuka said the Yamane technique requires the use of thin gauge needles (30 gauge) and long, oblique tunnels, but they are still prone to leaking. “On the extreme end of the spectrum,” they wrote, “Marfan patients or others with very long axial length have thin sclera and are considerably more prone to leaking. Additionally, we often do these cases combined with retina providers, whose ports may not consistently seal.”
Recently Dr. Nakatsuka had a patient with a completely collapsed eye after the procedure, which he thought was likely due to a small leak from a retina port in combination with aqueous suppression that can occur with ciliary body trauma. “Hypotony is a more frequently encountered complication and most often resolves as small leaks self-seal. However, long-term hypotony may lead to secondary complications, such as hypotony maculopathy. Initial medical treatment includes topical steroids, cycloplegics, or surgical closure of persistent leaks.”
Other complications: CME, ocular hypertension, iris trauma, and retinal trauma are common complications of any secondary lens replacement, regardless of technique, Dr. Pettey and Dr. Nakatsuka wrote. CME, they said, can be managed with topical NSAIDs and steroids or, if needed, intravitreal anti-VEGF or steroid injections.
The Yamane technique, according to Dr. Pettey and Dr. Nakatsuka, is susceptible to retained viscoelastic, which can cause elevated IOP. Dr. Nakatsuka has experienced this in up to 20% of cases and usually treats it prophylactically with oral acetazolamide or topical anti-hypertensives.
As for retinal trauma, Dr. Kim said if needles are positioned too posteriorly, in theory, they could pierce the peripheral retina and cause a retinal tear or detachment. Dr. Nakatsuka said extra care should be taken with small eyes that may have a shorter pars plana and a more anterior retina insertion leaving the retina vulnerable to puncture and trauma.
If there is retinal or corneal damage, such as a retinal tear, CME, or corneal endothelial decompensation, Dr. Kim said these conditions must be treated before IOL replacement or scleral refixation.
“As long as there is no permanent damage, when the IOL is replaced and scleral refixation is properly executed, the patient can have an excellent outcome,” Dr. Kim said, adding that he’s been referred patients like these and they have done well after surgery.

Source (all): Jeff Pettey, MD, and Austin Nakatsuka, MD
More advice on avoiding complications
Dr. Kim said it’s important to practice intrascleral haptic fixation on artificial eyes, by attending skills transfer courses, and/or by finding and working with an experienced mentor.
“I would also be cautious and selective when choosing which technique. Whether you try Dr. Yamane’s original technique or some other variant, ask yourself, does this cause undue stress on the haptics? Although the PVDF haptics are strong, they are not indestructible, so I would be wary of techniques that exert significant stress on the haptics. Are you having trouble with certain steps such as cannulating the trailing haptic? Find a safe technique that flattens the learning curve,” Dr. Kim said.
Dr. Kim said many surgeons have personalized the intrascleral haptic fixation technique with their own approach. He said he began using the Sensar IOL (Johnson & Johnson Vision) a few years ago when access to the CT LUCIA 602 was limited.
“With my modifications to the technique, I have been able to completely transition to the Sensar with excellent results despite the delicate PMMA haptics because of my gentle approach,” he said. “Since I use the Sensar and not the CT LUCIA 602 as my primary IOL, I have been able to avoid the recently described rotisserie optic tilt complication. The surgeons who adopted my techniques in response to this problem have informed me that it has helped them switch to the Sensar. To be clear, the PVDF haptics of the CT LUCIA are the most forgiving, thus the best IOL to use when learning the technique. However, once you master it, I would strongly advise trying other IOLs so you aren’t trapped with just one lens.”
About the physicians
D. Brian Kim, MD
Professional Eye Associates
Dalton, Georgia
Jeff Pettey, MD
Clinical Vice Chair
Moran Eye Center
University of Utah
Salt Lake City, Utah
Austin Nakatsuka, MD
Assistant Professor
Glaucoma/Cornea/Anterior Segment
Moran Eye Center
University of Utah
Salt Lake City, Utah
References
- Yamane S, et al. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology. 2017;124:1136–1142.
- Scoles D, Wolfe J. Laser to the Rescue. American Academy of Ophthalmology ONE Network. Dec. 15, 2022. www.aao.org/education/1-minute-video/laser-to-rescue-2.
Relevant disclosures
Kim: None
Pettey: Carl Zeiss Meditec
Nakatsuka: None
Contact
Kim: docdbk100@gmail.com
Pettey: jeff.pettey@hsc.utah.edu
Nakatsuka: Austin.Nakatsuka@hsc.utah.edu