Glaucoma: Complicated cases
September 2023
by Liz Hillman
Editorial Co-Director
The reason for MIGS, according to Manjool Shah, MD, is to address the gap that existed with the conventional paradigm in glaucoma management—the paradigm that had patients either on “safe” options, like drops or SLT, or facing higher-risk surgeries, like trabeculectomy and tube shunts, with little in between.
“The promise of MIGS is to fill that gap, specifically when it comes to safety,” he said.
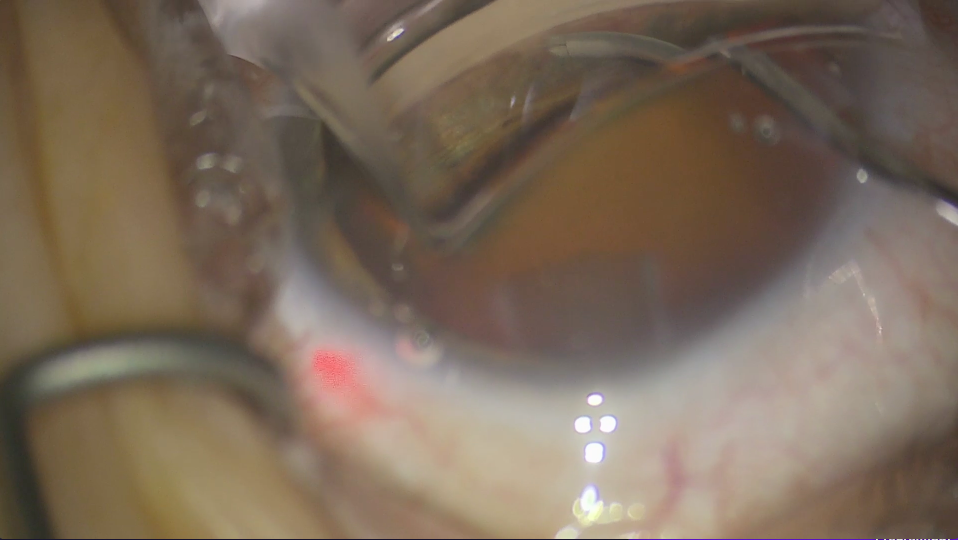
Source: Arsham Sheybani, MD
While MIGS do, for the most part, fulfill that promise, there can be complications during and after MIGS procedures that the surgeon needs to be prepared to identify and address.
Arsham Sheybani, MD, said that if you’re performing MIGS procedures, you should be able to address the common complications that occur without needing to refer the patient to another surgeon for management, at least not immediately. Dr. Shah agreed that management of many common MIGS complications are within the wheelhouse of those performing MIGS.
“If you can place the stent, if you can do the canaloplasty or the goniotomy, you’ve already performed the most nuanced surgical technique that day,” Dr. Shah said. “The hardest part of dealing with complications is recognition and choosing the appropriate intervention to manage it, and the management is completely in the skillset of those who perform the initial procedures.”
Complications with stenting MIGS
Dr. Shah said the most common complication with stenting MIGS, which in the U.S. include iStent (Glaukos) and Hydrus (Alcon), is malpositioning. “The key to success and safety with any angle surgery is visualization,” he said. “A good en face gonioscopic view will allow you to catch a misplaced stent easily.”
If you notice that the stent is in the wrong place, generally you can reposition it, Dr. Shah said, but he noted that the current iStent Inject only has a few clicks available with the current generation injector. This issue has been addressed with the newest generation iStent Infinite, which is rolling out across the U.S. Dr. Shah said reloading an iStent into the injector is a skill. “You might need to rethread it in the anterior chamber, then redeploy it, assuming you have more clicks at your disposal. If you run out of your four clicks, you can reposition an iStent manually using some microforceps, directly placing it where you need to or move it from point A to point B.”
Dr. Shah shared that over deployed iStents (usually caused by over dimpling of the cannula) can be repositioned with microforceps. To avoid under deployed stents, Dr. Shah advised applying a bit more force than you think you need, especially with the second stent.
With the Hydrus, the injector system allows you to remove and replace the stent as needed. Dr. Shah also noted the importance of a 15-degree upward angle of the cannula for proper Hydrus entry, as well as the importance of creating a separate paracentesis incision about 3–4 clock hours away from the area of planned stent insertion to allow the Hydrus to optimally match the curvature of the canal.
Bleeding (hyphema) is also a possibility with stenting procedures, as is damage that can occur due to contact with the iris root and/or ciliary body. There are two distinct bleeding patterns that surgeons need to be aware of with MIGS. One is a slow, focal, and normal amount of blood reflux. “A little blood reflux is a confirmatory sign that you’re in the right place, doing the right thing,” Dr. Shah said. This is in contrast to traumatic hyphema, which can occur due to inadequate visualization, abnormal anatomy, or patient movement that causes you to inadvertently touch or interact with the iris root or ciliary body. Dr. Shah said that this bleeding is more diffuse and at a higher velocity. He said cohesive viscoelastic should be used to tamponade this type of bleed, preventing more blood from entering the anterior chamber. The surgeon should also take the time to figure out what caused such hyphema and address it, if possible.
“Typically you’re going to have to move half a millimeter to a millimeter more anterior,” he said.
Dr. Sheybani said if a stent is placed in the wrong tissue plane, it doesn’t generally cause major intraoperative complications, again, unless it creates a cyclodialysis cleft. He clarified that something like the iStent is so small that even if it were accidentally placed in the suprachoroidal space, it probably isn’t going to cause an issue or significant bleeding. However, if the patient moves, the instrument doing the stent injection could create this damage. Dr. Sheybani also said that a misplaced stent could cause chronic iritis if it’s rubbing against structures it shouldn’t.
In the event of physical tearing or disinsertion of the iris or ciliary body, Dr. Shah’s recommendation is to leave alone a small iridodialysis. If it’s big, it may require repair, which Dr. Shah said is a specialized skillset.
Cyclodialysis cleft comes with a risk of postop hypotony. If it’s small, Dr. Shah said that a little postop inflammation can help seal it up and it will scar closed. Overall, though, if there is a cyclodialysis cleft, surgeons should monitor for postop hypotony, indicating a need for repair of the cleft.
Dr. Sheybani said small clefts should close on their own once the patient is off steroids.
Complications with the ‘otomies’ and ‘asties’
Dr. Shah said that hyphema and iridodialysis or cyclodialysis can also occur with goniotomy, trabeculotomy, and canaloplasty. With canaloplasty, Descemet’s detachment can occur. “It typically happens if we over inject viscoelastic in one focal area of the canal. That can cause the viscoelastic to track anteriorly, pulling Descemet’s off,” he said. “You’ll see lenticular mass in your field of view, which would be Descemet’s bowing down into the anterior chamber and the viscoelastic-filled space starting to occlude the anterior chamber.”
Dr. Shah said recognition of this situation early is key because it can then be easily managed. He said to cut down through the anterior cornea into that space, evacuating viscoelastic from an anterior approach and consider placing an air bubble to reapproximate Descemet’s.
Complications with bleb-forming MIGS
Though a bleb-forming procedure, XEN (Allergan) lives within the MIGS family, Dr. Shah said. Complications that can occur with XEN include malpositioning or unstable positioning, which Dr. Shah said is rare, and bleb-related issues.
Dr. Shah said there are a number of ways to place XEN (ab externo and ab interno), but the key is to make sure you have the right amount of the device in the anterior chamber and the subconjunctival space, and ensure that the “subconjunctival” portion is not enmeshed in Tenon’s.
In terms of bleb-related complications, these can include fibrosis, scarring, encapsulation, infection, and device exposure. These, Dr. Shah said, are less common with good surgical technique, appropriate use of anti-inflammatory agents, and careful management of the wound healing.
Dr. Sheybani said when you’re performing XEN with patients with very high pressures, the patient could be at risk for a suprachoroidal hemorrhage. Other possible XEN complications he mentioned were bleeding if you go through the iris root, conjunctival perforation from the insertion needle pushing through the conjunctiva, and Descemet’s detachment.
“Despite these things, in general, XEN intraoperatively is a very safe procedure. I tell patients they’re going to hear me talking about positioning and repositioning during the procedure because I want it perfect before we leave,” Dr. Sheybani said. “Repositioning at the time of surgery is not a worrisome thing for me because the intraop complications are so unlikely. … There is hypotony that can occur within the first 1–2 weeks, and there can be choroidals. There can be hyphema, less likely but possible. The advantage of XEN is that the long-term issues are less likely compared to the other filtration procedures.”
Prevention
In general, with all of these complications, prevention is key.
Here are some points Dr. Shah provided to help prevent complications:
- Make sure you’re choosing the right patients for any given procedure.
- Ensure you have an en face view for angle procedures and operate in reverse Trendelenburg.
- Know your landmarks, using trypan blue to stain the trabecular meshwork and Schlemm’s canal if needed.
- Use OVDs appropriately (a dispersive OVD to protect the endothelium and cohesive in the nasal angle); cohesive OVD can displace blood away from your view.
In his interview with EyeWorld, Dr. Shah also emphasized making sure incisions are watertight and potentially leaving a bit of cohesive viscoelastic in the anterior chamber for extra pressurization for eyes at risk of complications from decompression, such as choroidals or anterior chamber shallowing.
“To realize the promise of MIGS, we have to continue to put safety above all else. These procedures are safe when the proper steps are taken, when we take the time to get good visualization, when we recognize the right patient for the right process, when we’re meticulous with surgical technique,” Dr. Shah said. “The onus is on all of us as practitioners to maintain that high vigilance to be exacting in our technique, in our fundamental principles to live that promise that MIGS are meant to provide.”
About the physicians
Manjool Shah, MD
Associate Professor of Ophthalmology
NYU Langone Health
New York, New York
Arsham Sheybani, MD
Associate Professor of Ophthalmology and Visual Sciences
Washington University School of Medicine in St. Louis
St. Louis, Missouri
Relevant disclosures
Shah: Alcon, Allergan, Glaukos, Nova Eye Medical
Sheybani: Alcon, Allergan, Glaukos, Nova Eye Medical
Contact
Shah: manjool@gmail.com
Sheybani: sheybaniar@wustl.edu



