Cornea: Complicated cases
September 2023
by Ellen Stodola
Editorial Co-Director
W. Barry Lee, MD, and Elmer Tu, MD, spoke with EyeWorld about the risk of infections with lamellar corneal grafts, how patients may present, and how to handle this complication.
Any time a lamellar graft is done, whether it is an endothelial keratoplasty (EK) or anterior lamellar keratoplasty (ALK), an interface is created, Dr. Lee said. That interface has the potential to trap organisms and lead to a corneal infection. The most common interface infections occur from fungal organisms, particularly Candida species, Dr. Lee said. “Fortunately, lamellar graft infections are rare, but when they occur, they can be devastating,” he said, noting that Fontana et al.1 reported the rate of fungal infections after ALK is 0.052% and 0.022% after EK.
Source: W. Barry Lee, MD
Dr. Tu agreed that the most common infections that occur with lamellar corneal grafts are caused by Candida species. The rate of infection from the most recent 2022 data is approximately three infections per 10,000 endothelial grafts in the U.S. The true number is likely higher due to incomplete reporting, he said.
He added that infections are generally recognized at the 1-month follow-up appointment or later. “However, almost all infections are introduced at the time of surgery,” he said. When an infection becomes apparent, it is affected by the virulence of the organism, the number of organisms, and their location. Aggressive, high colony count, or peripheral/anterior chamber location contamination could become apparent in the first few hours or days after surgery, whereas the opposite may not become apparent for months. Rarely, late infections have been reported more than a year later, Dr. Tu said.
Interface infections can occur at any time after surgery, from a week after surgery to a year after, Dr. Lee said. Taking a fungal rim or media culture at the time of surgery can provide insight as to whether an organism is present on the donor tissue because infections are most commonly a result of transmission from the donor tissue.
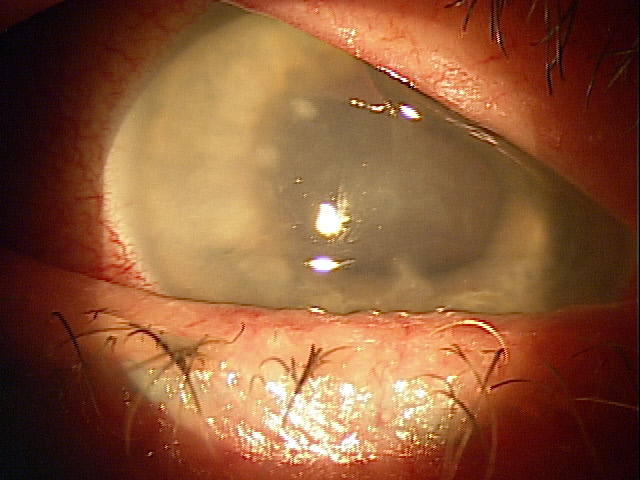
Patients typically present with decreased vision and occasionally discomfort and photophobia. “Initially, the eye tends to be quiet, but as the infection progresses, the eye becomes more red and irritated,” Dr. Lee said. “Slit lamp exam will often show a small white infiltrate in the interface of the cornea with anterior chamber cell and flare.”

Source: W. Barry Lee, MD
The majority of infections are asymptomatic or minimally symptomatic at the time of recognition, Dr. Tu said. As it advances, decreased vision, pain, and redness may occur. The infection usually presents with signs of inflammation, often subtle, as an isolated interface opacity but can present as an endophthalmitis, iritis, keratitis, or conjunctival inflammation.
In order to try to reduce the risk of infection, Dr. Tu said efforts have been focused on two areas: reducing/limiting transmission and prophylaxis. “A number of eye bank and surgeon practices have been implemented to reduce contamination, including additional antiseptic applications at the time of recovery, reiterating aseptic techniques, and minimizing tissue warming,” he said. “Exploration of adding antifungals to cold storage has not eliminated the risk. Post-surgical prophylaxis with antifungals has also been advocated but with minimal supporting evidence as to efficacy, medication, route, and dosing.”
Dr. Lee said that eye banks have provided the most effective way to prevent infections by changing the way they prepare donor tissue. “The Eye Bank Association of America has mandated that all tissues prepared for cornea transplantation undergo a double betadine prep, meaning the tissue is treated with betadine for a set period of time after it is procured, rinsed away, then another betadine exposure is applied to the tissue for a second treatment,” he said. “In addition, surgeons can now have the eye bank add antifungal medication to the tissue storage media.”
Once an interface infection is identified, patients should be started on topical treatment geared to the particular organism that was identified, Dr. Lee said. If it is a Candida infection, topical and oral antifungal medication should be started, along with consideration of intravitreal antifungal treatment. Some surgeons advocate interface injections of antibiotics or antifungals toward the infected area of the cornea.
Dr. Lee said that removal of the infected tissue is the next step. “For a Descemet’s membrane endothelial keratoplasty case, removal of the tissue should include intracameral antibiotic or antifungal injections,” he said. “If the infection is trapped in the interface and has not spread to the anterior chamber, a therapeutic keratoplasty may be warranted in a case of anterior lamellar keratoplasty or Descemet’s stripping endothelial keratoplasty.”
Additionally, Dr. Lee said that cultures of tissue or media at the time of surgery can be a useful guide for knowing what organism is present when an infection occurs. “The diagnostic dilemma remains what to do when you get a positive rim culture, as not all positive rim cultures progress to infection,” he said. Some surgeons prefer to start treatment with anti-infective agents as soon as a positive rim culture is reported while other surgeons do not treat and just watch the patient closely, he said, adding that no definitive treatment paradigm has been developed at this point.
Dr. Tu said that when treating these infections, topical and systemic antifungal treatment alone is associated with a high failure rate. Success has been reported with intrastromal injection, penetrating keratoplasty, and antifungals in conjunction with total or partial removal of the graft, he said.
Post-lamellar keratoplasty infections can have devastating outcomes with limited but potentially successful therapies, Dr. Tu said. Infections are rare but more common than with penetrating keratoplasty surgery. With limited clinical evidence for optimal management, practices should keep these factors in mind when deciding what interventions are appropriate and cost effective, he said.
About the physicians
W. Barry Lee, MD
Medical Director
Georgia Eye Bank
Atlanta, Georgia
Elmer Tu, MD
Professor of Clinical Ophthalmology
University of Illinois College of Medicine
Chicago, Illinois
Reference
- Fontana L, et al. Interface infectious keratitis after anterior and posterior lamellar keratoplasty. Clinical features and treatment strategies. A review. Br J Ophthalmol. 2019;103:307–314.
Relevant disclosures
Lee: Dompe, Glaukos, Sun Pharma
Tu: None
Contact
Lee: wblee@mac.com
Tu: etu@uic.edu



