Refractive: Lessons learned
December 2023
by Ellen Stodola
Editorial Co-Director
Lens tilt or decentration can occur with intraocular surgery, and while not always something that physicians need to address, this may require attention with more complicated cases or with larger decentrations. A physicist and a physician discussed what they look for and techniques that might be used.

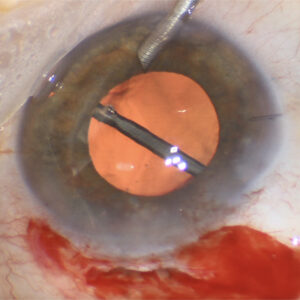
Source: Brandon Ayres, MD
The eye is a very non-aligned system, said Susana Marcos, PhD. The fovea does not align with the optical axis of the eye. Even the optical components of the eye (cornea, crystalline lens, and pupil) are not aligned with respect to each other. “In the majority of cases, the tilt or decentration of the lens does not result from surgery but from the natural misalignment of the capsular bag,” she said, adding that preserving the natural misalignment is generally a good thing.
Dr. Marcos said that she and colleagues generated computer models of pseudophakic eyes using anatomical information and the intraocular lens geometry, including tilt and decentration of the lens, obtained using fully quantitative 3D anterior segment imaging. The wavefront aberrations measured matched measurements from aberrometry when tilt and decentration were included. “We found that in 75% of the cases, having the small amounts (and orientation) of the tilt and decentration produced slightly better quality than having zero tilt and decentration. In a sense, the tilt and decentration of the lens tend to compensate [for] the effects of the off-axis position of the fovea.”
There are a number of techniques to measure tilt and decentration of the lens (before and after surgery) and estimate the effect on retinal image quality, Dr. Marcos said. Her lab has developed techniques based on Purkinje imaging,1,2 Scheimpflug imaging,1 and most recently, on OCT to measure tilt and decentration of IOLs in vivo.3,4 “With 3D quantitative OCT, we can measure corneal topography (anterior and posterior), lens and fovea alignment, and construct eye models,” she said. “Those techniques do not prevent tilt and decentration from happening but certainly can quantify the effect on image degradation.”
When deciding whether action is needed to address lens tilt or decentration, Dr. Marcos said this will likely depend on the optical design of the lens. Other factors to consider are corneal aberrations. Using patient-specific computer eye models (based on measured topography and biometry), it is possible to test the effect of tilt and decentration on the retinal image quality and predict the impact on vision, she said.

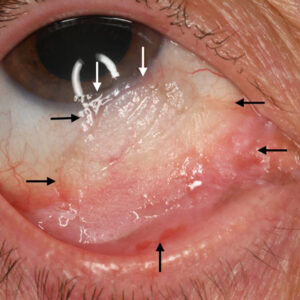
Source: Brandon Ayres, MD
Lens tilt and decentration can be a broad spectrum, according to Brandon Ayres, MD. It runs the gamut of a little bit of decentration due to an asymmetric capsulorhexis all the way to a tilted suture-fixated lens that induces 4 or 5 D of astigmatism.
When thinking about tilt and decentration with standard monofocal lenses, Dr. Ayres said this is something that can be seen but is not usually a major concern. With some of the more advanced technology lenses, the aspheric IOLs especially, if they begin to decenter, there may be a decrease in quality of vision. If there’s a capsule complication and you can’t get the lens in perfectly centered or if there’s asymmetric phimosis or scarring of the capsule, it can cause a decrease in visual quality. There’s less of an issue optically if you’re using a non-aspheric or a zero asphericity lens, Dr. Ayres said. If there are small amounts of decentration due to patient healing, it’s not going to impact quality of vision as much.
“I don’t lose too much sleep over decentration of standard IOLs because it’s not a major problem,” he said. There are a variety of implant options now available. Some are zero asphericity and some transition from negative to zero asphericity depending on where you are in the lens.
Risk factors for decentration include a discontinuous capsulorhexis, a small capsulorhexis, a decentered capsulorhexis, if you can’t get a good overlap of the anterior capsulorhexis with the IOL, and patients who are more prone to capsular phimosis like those with pseudoexfoliation or high myopia.
In uneventful cataract surgery, Dr. Marcos finds that standard IOL platforms preserve, to a large extent, the tilt and decentration of the natural bag, though she noted that this does not include complications like dislocation and zonular weakness. “We also found a larger amount of tilt in eyes implanted with lenses with hinged haptics,” she said, adding that these lenses did not preserve the orientation of the preoperative capsular bag.
Dr. Marcos does not see a huge concern for these issues in standard cataract surgery, but she said it’s important for surgeons to anticipate when they might have a complicated surgery. This includes patients with a history that makes them likely to have zonular weakness, like severe pseudoexfoliation, high amounts of myopia, a history of trauma, or Marfan syndrome.
“Specific lenses may exhibit designs that make them critical to align with the pupil center,” Dr. Marcos said. “To my knowledge, most designs have some tolerance to the amount of tilt and decentration in normal cases (<0.5 mm, <5 degrees), but in some cases, haptic designs could be envisioned to ensure centration.”
Extreme decentration, in Dr. Ayres’ experience, is usually due to capsular phimosis. “The times I’m dealing with this are when there is capsular phimosis shortly after cataract surgery. I’m very quick to do a YAG laser and relax the anterior capsule by doing anterior capsular polish, which is basically a YAG capsulotomy to the anterior capsule to break the phimotic or scarring ring.” This lets the implant settle in a better position, he said.
“It’s not that common with a monofocal lens that I’m going back to the operating room to recenter it,” Dr. Ayres said. “However, in a toric IOL or multifocal IOL that’s decentering, and we think that decentration is causing a decline in quality of vision, that’s different. There we will go back to the operating room and reopen the capsule and try to rotate the lens, if necessary, or reposition the lens so that it’s better centered because that little bit of decentration, especially with the diffractive multifocal, makes a difference and you can see a rapid decline in quality of vision.”
Toric IOL rotation is going to happen in some patients, Dr. Ayres said, whether it’s due to retained ophthalmic viscosurgical device, the patient rubbed their eye, or the patient has a larger eye than average or is a high myope.
If you know someone is at risk for decentration, you have to be more proactive, Dr. Ayres said. For example, if you’re operating in a high myope, some physicians would place a capsular tension ring (CTR) to prevent decentration or to have equatorial forces out to reduce scarring and phimosis, and that may help with the IOL staying centered. It’s also important to make sure you are appropriately sizing and positioning the capsulorhexis. A tool like the femtosecond laser where you can be very precise or the ZEPTO IOL Positioning System (Centricity Vision), which makes a precise, round capsulorhexis, may help, he said.
Some patients may experience a major decentration, rather than just a minor issue. These major decentrations would likely come from a surgical complication, Dr. Ayres said, like a severe zonulopathy or posterior or anterior capsular tear. Patients may notice reduced vision, double images, or dysphotopsias due to reflections off the edge of the lens implant.
“The problem we have is fixing that IOL or replacing it with a new lens using an alternative technique, the common one being the Yamane technique or some other form of scleral-fixated IOL. The decentration and tilt are still a problem, and we’re placing a lens in the absence of capsular support, and there is not a device or IOL that is specifically made for and designed for non-capsular placement,” Dr. Ayres said. “We do all sorts of measurements preoperatively and in the operating room, trying to pick the best technique for that patient. At the end of those surgeries, sometimes you look through the microscope, and even with all the measuring, it still looks a little decentered or tilted, and the repair for that can be difficult.”
In addition, Dr. Ayres said, all the techniques used are technically off label. “We have very good techniques, but they’re less accurate when it comes to biometry, and it’s easier to get decentration and tilt.” Patients are already worried about their vision and know they have a complex ocular problem. The fear and frustration level escalates when in some cases patients need to return due to decentration of the implant. Proper counseling and a good doctor-patient relationship is required to maintain trust in these situations.
In addition, it’s your responsibility to manage both the patient’s condition and help the referring physician manage their relationship, Dr. Ayres said. Many times you’re starting out with a frustrated patient, so it’s important to try to and improve the patient’s outcome and inform them that there is no cookbook recipe for managing complex problems. Even the best surgical solutions may have complications and frustrations.
Decentration problems can occur both immediately after surgery or down the line, Dr. Ayres said. He gets calls from doctors during surgery or postop day 1 trying to get the patient a follow-up visit to manage the situation. There are also late dislocations, where the surgery 20 years ago was fine and now there’s a zonulopathy (maybe the patient had a vitrectomy or has pseudoexfoliation), and the current lens is dislocating or tilted. In these cases, we’re either trying to reposition the existing lens or exchange it for a new one, Dr. Ayres said, which would have to be an anterior chamber lens or an IOL fixated to the sclera, and you run into the same challenges trying to ensure the new lens is properly centered without tilt.
ARTICLE SIDEBAR
Lessons learned
Kevin M. Miller, MD, Cataract Editorial Board member, shared a lesson he has learned to “level up”:
I have increasingly come to appreciate a facet of human behavior that is on full display before and after surgery, especially cataract and refractive surgery. It is that the patient’s frame of reference changes after surgery.
What would have been a 1 or 2 complaint on a 0–10 scale before surgery becomes an 8 or 9 after surgery. People quickly forget how badly they had it before surgery, and the little things that didn’t bother them all that much before surgery suddenly become “big problems” after surgery. Surveys are where you see this behavior on display the most.
I have been involved in multiple artificial iris device trials. We always rate photosensitivity, glare, halos, etc., before and after surgery. There is no question that iris devices help reduce all these symptoms. Someone may state their symptoms are a 7 out of 10 before surgery and a 6 out of 10 after surgery. How can that be?
I remind them: “You said your symptoms were a 7 out of 10 before surgery, and now they are a 6 out of 10. So the surgery and iris device didn’t help you that much, correct?” The patient will say, “No, I am much better off now. I’m so happy I had the surgery!” Then I ask, “If you were a 7 before surgery, what are you now?” The patient will answer, “Maybe a 0 or 1.”
This frame of reference change happens all the time. In order to get at the truth, we need to remind patients how they rated their symptoms (or how bad their vision was without glasses, how poor their reading vision was, etc.) before surgery. Otherwise, they confuse you by subconsciously changing their frame of reference.
About the doctors
Brandon Ayres, MD
Co-Director of the Cornea Fellowship Program
Wills Eye Hospital
Philadelphia, Pennsylvania
Susana Marcos, PhD
Professor
Department of Ophthalmology
University of Rochester Medical Center
Rochester, New York
References
- de Castro A, et al. Tilt and decentration of intraocular lenses in vivo from Purkinje and Scheimpflug imaging. Validation study. J Cataract Refract Surg. 2007;33:418–429.
- Rosales P, Marcos S. Phakometry and lens tilt and decentration using a custom-developed Purkinje imaging apparatus: validation and measurements. J Opt Soc Am A Opt Image Sci Vis. 2006;23:509–520.
- Marcos S, et al. Three-dimensional evaluation of accommodating intraocular lens shift and alignment in vivo. Ophthalmology. 2014;121:45–55.
- Sun M, et al. Intraocular lens alignment from an en face optical coherence tomography image Purkinje-like method. Opt Eng. 2014;53:061704.
Relevant disclosures
Ayres: Alcon, Bausch + Lomb, Carl Zeiss Meditec
Marcos: Co-inventor in patents for anterior segment OCT quantification, crystalline lens shape measurement, and estimated lens position from OCT
Contact
Ayres: BAyres@oppdoctors.com
Marcos: smarcos2@UR.Rochester.edu