Cornea: Lessons learned
December 2023
by Ellen Stodola
Editorial Co-Director
According to Lisa Nijm, MD, JD, neurotrophic keratitis (NK) is still considered a rare disease, but she thinks that it occurs more often than many realize. “It’s difficult to isolate the exact prevalence because so many times there is a delay in diagnosis. We might not even realize in the early stages that the patient has NK, and that’s what’s contributing to their poor healing.”

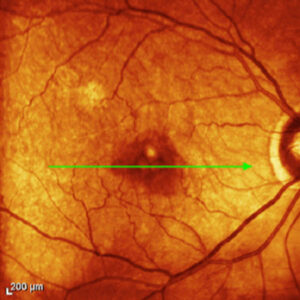
Source: Francis Mah, MD
While NK isn’t something that you necessarily see daily in a busy tertiary care cornea practice, Francis Mah, MD, said he sees it a couple times a week. It can be a patient with trauma or an abrasion, or a patient who just had surgery and is taking a couple of extra days to heal.
“[There is] this category we call persistent corneal epithelial defects, and in somewhere between 30–60% of them, the reason they’re not healing is NK,” Dr. Mah said. “It’s important to decide why the patient is not healing because it’s not normal for a patient to walk around with a persistent corneal epithelial defect.”
He added that it’s important to ask the patient about their history to figure out what might have predisposed them to this. Herpes simplex and herpes zoster are the most common reasons for NK, Dr. Mah said, but it also could be a history of trauma, a recent infection, or a chemical injury. “Getting the history and starting the thought process for why this person’s cornea isn’t healing is the first step.”
Once you have the history and find, for example, the patient has diabetes, a history of herpes or shingles, they had LASIK, or they have been on eye drops for a long period of time, you might start wondering about NK. You would then want to do corneal sensitivity testing, Dr. Mah said, either qualitative or quantitative. Testing could involve taking a cotton swab and pulling out the cotton part a bit and testing the patient’s sensation. “Corneas are exquisitely sensitive, so if the patient responds, that’s normal,” he said. “If they don’t respond or it’s delayed, that’s a little abnormal.”
Dr. Nijm also pays particular attention to a patient’s history in considering NK. Long-term contact lens wear is something specifically to look for because many patients begin contact lens wear in their teens and are coming in 50 or 60 years later; that’s a long time to be wearing contact lenses, and the effects on the cornea and the cornea nerves can manifest as NK, she said. She added that factors like diabetes, MS, and acoustic neuroma or meningiomas may also play a role and reduce corneal sensitivity.
Dr. Nijm agreed that the easiest and fastest test for corneal sensitivity is with the use of a cotton swab. She said to be sure to test both eyes and look for patients’ blink to stimulus. A more formal test that can be used is the esthesiometer, which can allow a numeric assessment, looking at different quadrants.
“As dryness and corneal sensitivity often go hand in hand, I also observe the blink rate and tear breakup time, and I’ve come to use osmolarity more frequently to help distinguish dry eyes from other potential causes of inflammation on the ocular surface that might mimic dry eyes,” Dr. Nijm said. “If I see the osmolarity is high, I will also look more carefully at corneal sensation. Studies have shown that over time, high osmolarity will cause damage to corneal nerves.”

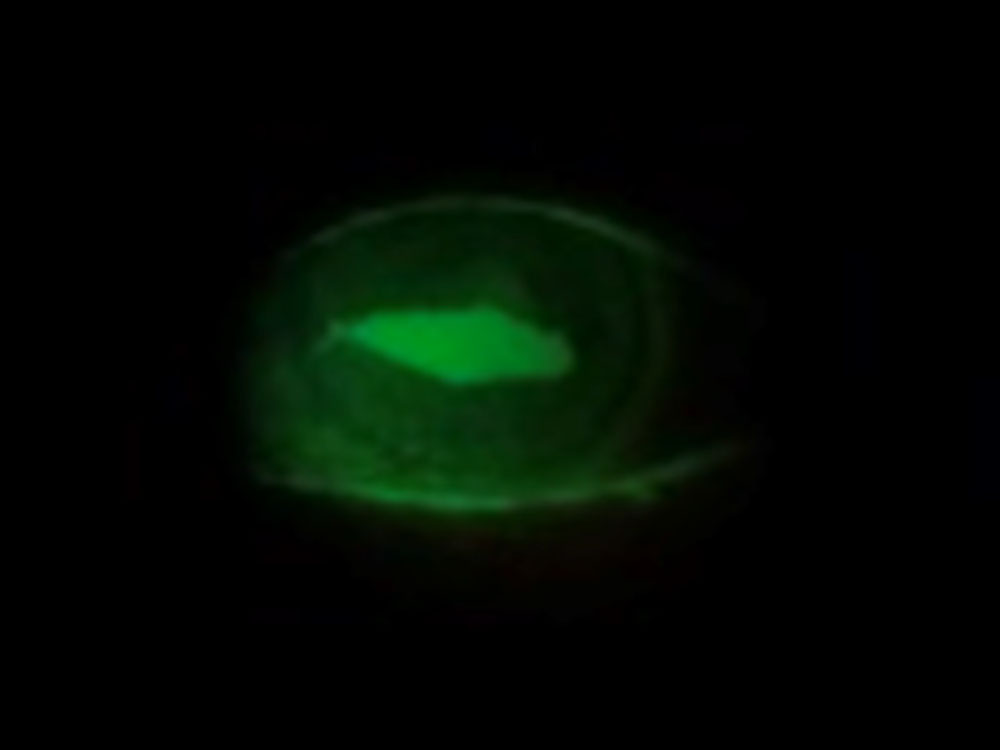
Source: Francis Mah, MD
There are many treatment options available for various stages of NK. It can be simply eliminating some of the factors that are preventing the healing, Dr. Mah said. If the patient is on glaucoma medications as well as medications for dry eyes, decreasing the overall volume of preservatives is going to be helpful.
Environmental factors are also important to consider. These can include ceiling fans, air blowing on their face, computer use, etc. Dr. Mah said lowering the screen or having them blink more frequently can be helpful.
Patients can use preservative-free lubricants, like artificial tears, gels, or ointments, Dr. Mah said, reiterating the importance of limiting preservatives. “We then typically go to a bandage contact lens,” he said. Allowing a lot of oxygen through the contact lens is helpful, and he likes to prescribe a preservative-free antibiotic eye drop when using a bandage contact lens.
The next thing you would typically think of is either serum tears or platelet-enriched growth factor, or an amniotic membrane. “After that, we’re thinking about Oxervate [cenegermin- bkbj, Dompe],” he said.
“The first time I see a patient, I’m wondering what they’ve done or haven’t done,” he said. Dr. Mah said he might jump to a bandage contact lens in the office, or he might try Prokera (BioTissue). Because Oxervate can take a while to get, he might start the ball rolling for that.
“[For] Stage 1 of the Mackie classification, where there’s alterations of the corneal epithelium that shows some SPK, I usually start with some type of increased lubrication, ointments, or preservative-free tears,” Dr. Nijm said. If there’s progression or it’s someone who is closer to Stage 2, she would consider adding punctal plugs and/or topical antibiotic to decrease the likelihood of infection. She considers the use of amniotic membrane and cenegermin-bkbj treatment as well. Dr. Nijm said she prefers to be aggressive at early stages to get the cornea to improve as quickly as possible because it’s preferable to prevent further progression or a perforation.
If these treatment options don’t work, Dr. Nijm said tarsorrhaphy is an option. Scleral contact lenses and autologous serum drops are also useful, she said.
Patients have to be watched carefully. You need to stop progression of the defect, she said. “Identifying it earlier and being more cognizant of the different treatment options will hopefully decrease the number of patients who reach Stage 3,” she said.
Corneal neurotization is also an option that may address the underlying concern. “It’s a complex surgery that requires dedication from corneal and plastics teams and something that is performed typically only in academic institutions,” Dr. Nijm said.
Dr. Nijm said she will choose to move forward with treatment quickly if the cornea isn’t going in the right direction. Neurotrophic corneas often remain neurotrophic; even if the ulcer heals, it’s possible that the underlying problem remains. If patients have had neurotrophic ulcers in the past, they are high risk, so it’s important to start treatment right away to prevent further complications.
It’s also important to educate patients to look for the signs. “They don’t have feeling, so they may not be aware of how bad their eye is. It’s important for the patient to be aware if their vision gets blurry or if the eye is red,” Dr. Nijm said. “We don’t want them to wait for a large ulcer to develop.”
“Patient education on preventative care is critically important, as well as the need to come back sooner to the office if they see any changes because they won’t feel the changes the same way someone else would.”
Lisa Nijm, MD, JD
Maintenance therapy is also important. “I make sure all my NK patients have their dry eye well treated, and they continue to use lubricants and anti-inflammatories as needed on a long-term basis,” she said. “Patient education on preventative care is critically important, as well as the need to come back sooner to the office if they see any changes because they won’t feel the changes the same way someone else would.”
Dr. Mah said NK is becoming transitional in terms of what stage you see because there is so much education out there. “I think 5 years ago, we weren’t making the diagnosis as early because there wasn’t a specific treatment. Therefore, by the time we made the diagnosis, I was seeing more advanced cases, where patients had some corneal melting or they had the persistent epithelial defect for weeks to months,” he said. “Now, because a lot of education is out there, I’m seeing less Stage 3. Patients are being identified, diagnosed, and referred much sooner.”
He also thinks physicians have become more sensitive to NK earlier. This might include testing patients who don’t necessarily have an epithelial defect, such as Stage 1 NK patients who look like they have dry eyes or have a history of unresponsive or recalcitrant dry eye or keratitis. “I think the word has gotten out, and the education has been helping patients in terms of getting identified sooner.”
As to whether NK can be cured, Dr. Mah said one question to ask is, “Can I get this person healed?” He noted that studies with Oxervate have shown that 70–75% of patients were healed within 8 weeks of their treatment. In terms of more traditional treatments, it’s still possible for patients to heal, but the problem is that most treatments—like eliminating preservatives—don’t address the root cause, Dr. Mah said. “They don’t reverse the lack of corneal sensitivity or sensation.”
He added that in the broader picture of persistent corneal epithelial defects, the success of a product like Oxervate addresses an unmet need, and its success encourages other companies to pursue products to address this. “I think there will be more companies out there looking at the same indication,” he said.
About the physicians
Francis Mah, MD
Scripps Clinic
La Jolla, California
Lisa Nijm, MD, JD
Warrenville Eyecare & LASIK
Warrenville, Illinois
Relevant disclosures
Mah: Dompe, Kala Pharmaceuticals
Nijm: Dompe
Contact
Mah: Mah.Francis@scrippshealth.org
Nijm: LMNijm@uic.edu