Cornea: Hot topics in ophthalmology
December 2022
by Ellen Stodola
Editorial Co-Director
The push for widespread COVID-19 vaccination has renewed the focus on the side effects that vaccines may have. It’s an especially unique situation due to the distinct timeframe for this mass vaccination campaign. Clara Chan, MD, and Bennie H. Jeng, MD, spoke about potential ocular impacts of the vaccine and what physicians should look for.
The concept of vaccine-induced corneal graft rejection, or any ocular inflammation, is not new, Dr. Jeng said. “Long ago, people wondered if a flu vaccine or any other vaccination can trigger an immune reaction,” he said. “It makes sense because the vaccination boosts your immune system, and your immune system gets revved up.” Previously, physicians were more likely to see random case reports, but it is appearing more now because of the worldwide push for a higher percentage of people to get COVID-19 vaccinations in a relatively short timeframe. “With a corneal graft, there is something antigenic in the eye, and the vaccination boosts the immune system, potentially causing the immune system to go after the transplant,” Dr. Jeng said. However, he said, “it can be very hard to prove causation in these cases.”
Timing wise, if a patient has a graft that’s been doing fine for 6 years, they get the COVID-19 vaccine, and a few weeks later there is a rejection for the first time, that’s suspicious, Dr. Jeng said.
While Dr. Jeng said he hasn’t experienced any of these cases in his practice, there have been multiple reports in the literature. “My patients ask me, because I think they have heard about the possibility, ‘Is it OK if I get the COVID-19 vaccination?’ My answer is ‘You should get it, and if it causes graft rejection, we can treat that and usually get you over it.’”
There are some doctors who will start upping patients’ steroids for a couple of weeks before the vaccination and continue for a couple of weeks after, then bring them back down to potentially protect against any reaction. There are others like Dr. Jeng who will just have patients call immediately if there are any reactions after the vaccine. These reactions could include red eye, light sensitivity, pain, and decreased vision, among other symptoms. Dr. Jeng prefers the latter approach because adverse reactions are infrequent, so you may be overtreating 500 people to catch one. Additionally, most of the time if you treat after the fact, you can get patients through the episode with successful graft survival, he said.
While you can’t always plan for when patients get their vaccine, Dr. Jeng said that if given the choice, he would recommend they get the vaccine before having a corneal transplant. If there is a chance that the vaccine could cause rejection, it’s potentially a lot of resources wasted.
Source (all): Clara Chan, MD
Dr. Chan presented on the topic of vaccination and the possibility of graft rejection during the Lindstrom Symposium at the 2022 ASCRS Annual Meeting. In her presentation, titled “Are We Seeing More Inflammatory Corneal Events?,” she shared cases she has encountered of corneal complications after COVID-19 vaccination. Because of the pandemic, Dr. Chan said there were a number of variables to consider: A lot of patients missed their follow-up appointments; prescriptions were not being renewed; there was a fear of steroids causing “immune compromise”; there was a fear of coming to the hospital clinic “where COVID patients go;” and there was a push for mass vaccination.
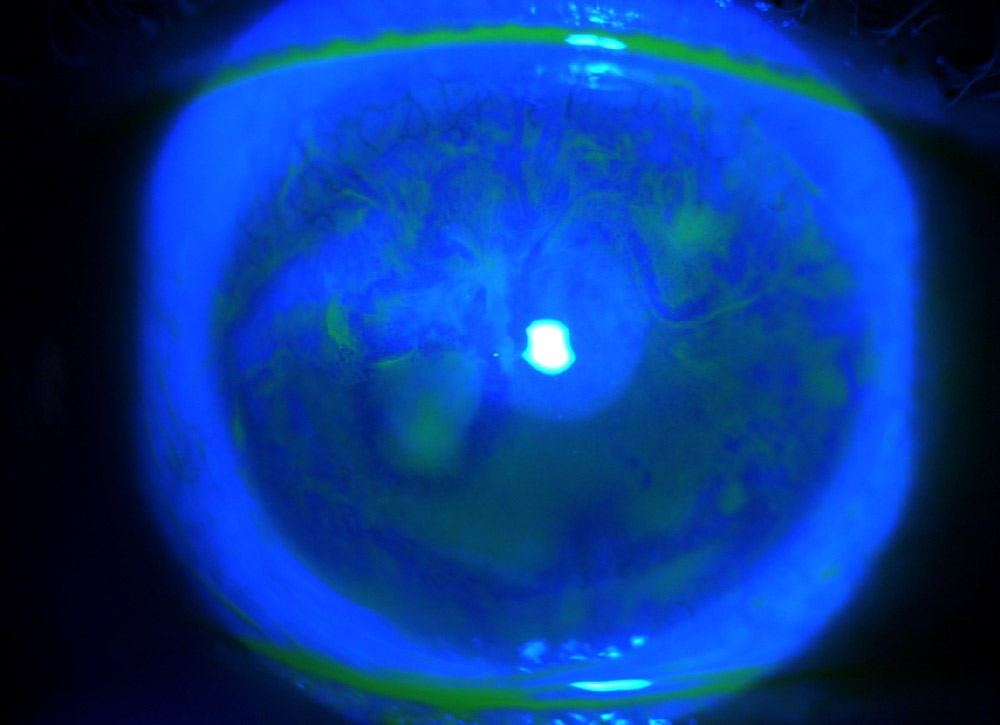
The first case Dr. Chan shared was that of a DMEK rejection in a 69-year-old male. The patient had his first DMEK in 2019 for Fuchs dystrophy in the left eye, and it was a routine surgery. However, the patient stopped his steroid drop. Rejection led to DMEK failure, persistent corneal edema, and vision down to 20/200.
In 2020, the patient had his second DMEK in the same eye, which was an uneventful surgery. Dr. Chan said he was doing fine postoperatively, but 4 months later came in complaining of a red eye. The patient reported symptom onset about 3 weeks after his first dose of the COVID-19 vaccine. Given his history, Dr. Chan was more aggressive and added oral steroids as well as topical. He was on prednisolone and cyclosporine, and BCVA was 20/40. Dr. Chan increased topical steroids, which resolved the symptoms.
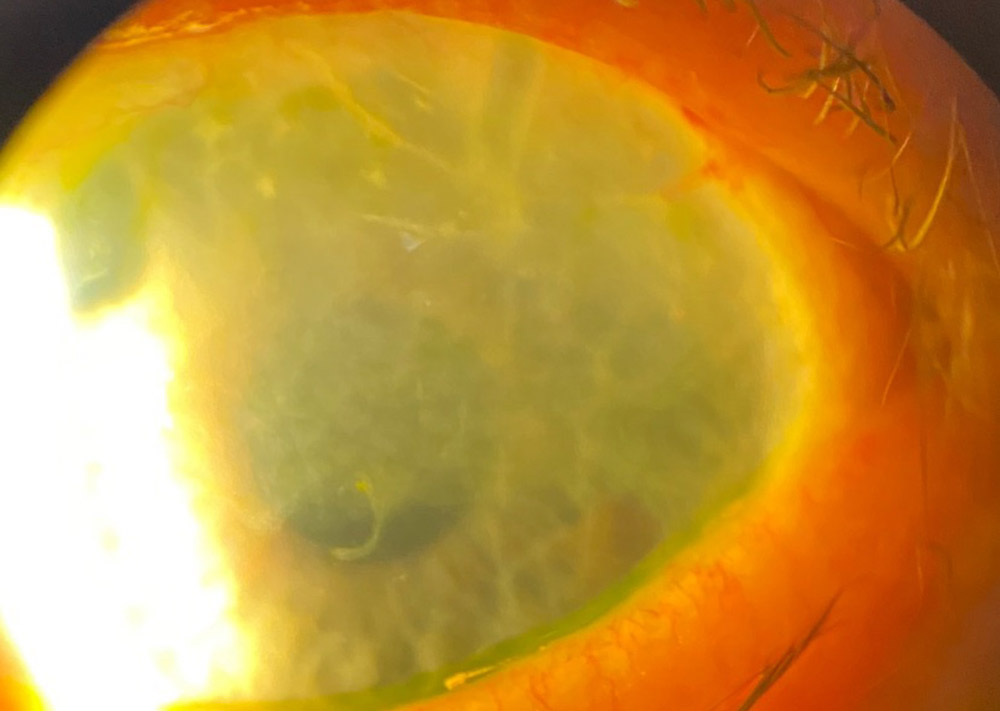
Her second case was that of a keratolimbal allograft rejection in a 73-year-old patient who had been stable for the last 6 years. There had been a lot of work done with this patient’s eye to reconstruct it because he had stem cell disease. He had undergone keratolimbal allograft, stem cell transplant from a deceased donor. Then he had a penetrating keratoplasty and cataract surgery. The patient had total limbal stem cell deficiency (LSCD) from a chemical injury before treatment.
He had baseline UCVA 20/60 and was on cyclosporine, dorzolamide/timolol, brimonidine, prednisone, and oral tacrolimus. He was doing great, Dr. Chan said, but came in 3 weeks after the first dose of his vaccine and had engorged vessels in each of the keratolimbal segments. Dr. Chan had to be very aggressive and stepped up topical steroids and systemic immunosuppression. The patient refused to take oral prednisone due to a fear of steroids, making him further immunosuppressed.
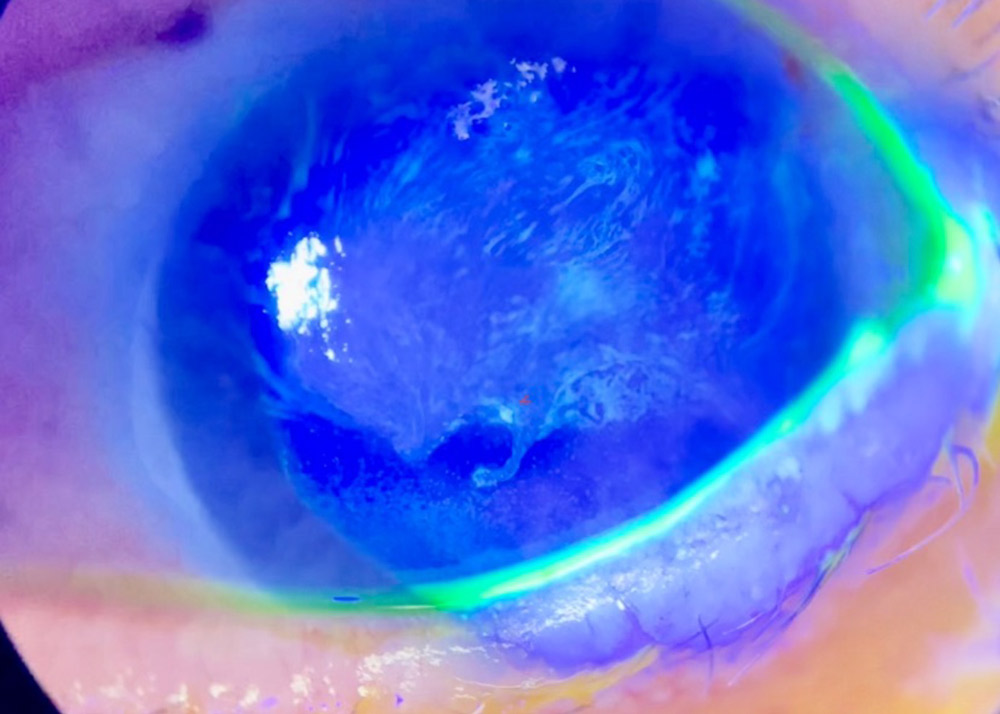
Her third case was that of an 81-year-old female with HSV immune keratitis flare and LSCD progression. She had stable BCVA 20/50 for 5 years. She received dose two of the vaccine 2 weeks prior to complaints of a red eye and decreased vision. She presented with counting fingers, AC 1+ cells, corneal edema, and active haze. Dr. Chan said the cornea was severely inflamed, so she bumped up topical steroid and oral antivirals.
A month later, the corneal swelling had cleared, but her LSCD progressed further. Whorl-like late staining passed beyond the pupil, and vision was decreased permanently. But Dr. Chan noted that her other eye was good, so the patient didn’t want anything done.
The final case Dr. Chan shared was that of a 54-year-old male who was stable with medically managed Crohn’s disease. He had recent shingles immune stromal keratitis 3 months prior and was on valacyclovir and loteprednol. He was still somewhat immunocompromised but was stable. The patient complained of pain, redness, tearing, and blurry vision OD 2 weeks after getting the vaccine. He had a flare-up of shingles immune corneal keratitis. Dr. Chan stepped up his steroid, and a week later, the corneal edema had unusual dendritic-like epithelial lesions. Given the history of cold sores, she thought it was a herpes simplex complication or zoster. Dr. Chan had to balance the topical steroid with oral antiviral coverage. Eventually, she was more aggressive with treatment for this patient and added topical ganciclovir, as well as amniotic dehydrated membrane and acyclovir ointment. Two months later, she was able to get the patient back to a baseline of 20/50 vision.
Dr. Chan said for the first time in history, there is an mRNA vaccine that delivers specific genetic information to host cells to produce foreign proteins, which leads to the immune system being upregulated. Inflammatory events have been reported with all of the different COVID-19 vaccines. There are still unknowns about the mechanism of action of these vaccines, she said, so it’s important for physicians to pay attention when asking patients about any inflammatory reactions and acknowledge when the last COVID-19 vaccine was.
“I have counseled patients about the signs and symptoms of ocular inflammation,” she said. She recommends transplant patients get the COVID-19 vaccine series prior to their transplant and recommends a baseline prophylaxis dose in high-risk grafts.
About the physicians
Clara Chan, MD
Associate Professor
Department of Ophthalmology and Vision Sciences
University of Toronto
Toronto, Canada
Bennie H. Jeng, MD
Professor and Chair
Department of Ophthalmology
University of Pennsylvania
Perelman School of Medicine
Philadelphia, Pennsylvania
Relevant disclosures
Chan: Johnson & Johnson Vision, Novartis, Santen
Jeng: GSK, Oyster Point Pharma, Santen
Contact
Chan: clarachanmd@gmail.com
Jeng: Bennie.Jeng@Pennmedicine.upenn.edu