News & Opinion: Tools & techniques
May 2012
by John A. Hovanesian, M.D., and Andrew Behesnilian, B.S.

Besides cataract surgery, pterygium excision is perhaps one of the most common surgical procedures for the general ophthalmologist. When performed as an excision alone, recurrence rates can be as high as 40% with aggressive and restrictive tissue replacing the primary pterygium. Past attempts at reducing recurrences with radiation or chemotherapy have resulted in long-term scleral melting and serious morbidity. The current standard for treating pterygium involves the use of conjunctival autografting, but amniotic membrane is also being utilized in place of conjunctival grafts with success. The most cost-effective means of treating pterygium would be to use the patient’s own conjunctival autograft secured in place with nylon sutures, however, there is increasing utilization of fibrin glue in these procedures that appears to reduce the inflammation caused by sutures while improving surgical efficiency.
In this month’s column, John A. Hovanesian, M.D., describes an alternative technique for pterygium excision that utilizes both amniotic membrane and a conjunctival autograft, both secured with fibrin glue. As with most of the articles in this column, it is not the only means or the simplest means of removing pterygium, but it does offer an alternative method that I believe you will find interesting. His step-by-step approach for working with fibrin glue will be valuable for any surgeon wishing to convert to this method of grafting.
—Richard Hoffman, M.D., Tools & techniques editor
Using conjunctival autograft and prophylactic subconjunctival placement of amniotic membrane
Introduction
Pterygium surgery using a conjunctival autograft is associated with recurrence in 5% of cases.1 These recurrences arise from the subconjunctival Tenon’s fascia surrounding the autograft. Amniotic membrane transplantation (AMT) has been used as an ocular surface graft in place of the conjunctival, but recurrence rates are similar to eyes receiving autografts.2 This is possibly because the amnion wears away from the ocular surface within 2-3 weeks of surgery and does not provide its well-known antifibrotic effects in the subconjunctival space from which recurrence is known to arise.
We devised a method where AMT is used prophylactically as a biologic implant beneath the conjunctiva surrounding the autograft (and not beneath the autograft itself). In this location, protected from the ocular surface, the AMT may provide more prolonged antifibrotic effects. A series of 40 pterygia undergoing the procedure described below were followed a mean of 10 months (range 4-17) with no recurrences.3




Source (all): John A. Hovanesian, M.D.
Anesthesia
Anesthesia is achieved with a peribulbar block of bupivicaine and lidocaine 1% with epinephrine. Subconjunctiva infiltration is also effective for the procedure but in our experience allows more post-op discomfort.
Step-by-step surgery
Fibrin tissue adhesive (Tisseel, Baxter Healthcare, Deerfield, Ill.) is reconstituted according to the manufacturer’s instructions, but the solutions are not transferred to the supplied Duploject syringe. Instead, they are left in their original vials.
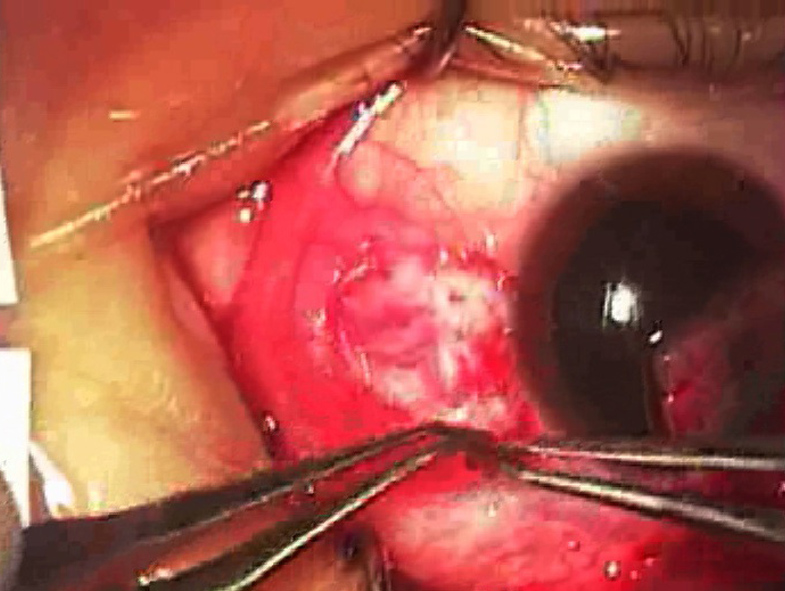
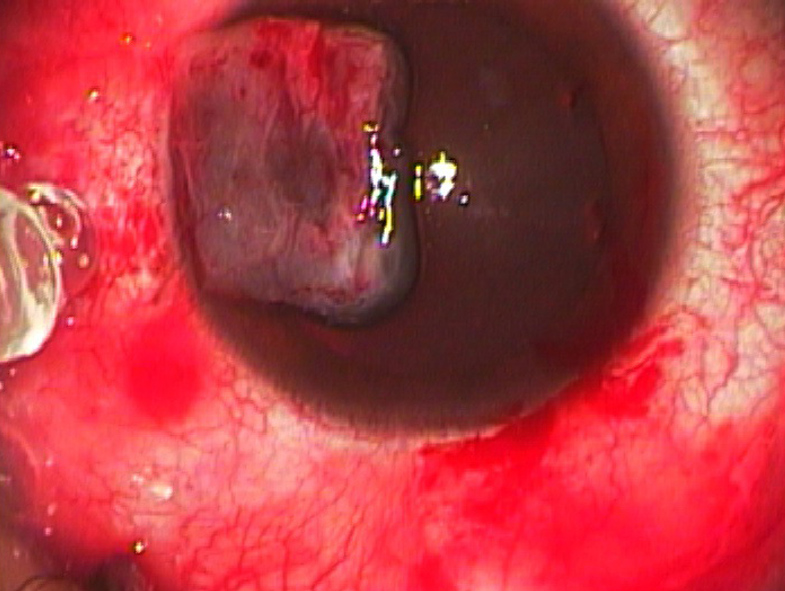
The pterygium is excised along with a conservative (about 1 mm) margin of healthy conjunctiva, leaving a conjunctival defect and exposed bare sclera (Figure 1). Next, blunt Westcott scissors are used to create a potential space about 5 mm beneath the healthy conjunctiva on the three sides surrounding the excision site. This potential space should be superficial to most of Tenon’s fascia and to the medial rectus muscle and tendon. Cautery is used conservatively (see Pearls). From the superior limbus, a thin conjunctival autograft is prepared, bringing along minimal Tenon’s fascia. The graft should be sized similar to the conjunctival defect. At this point, the graft is left attached (Figure 2) at the limbus superiorly so it is not misplaced during the following steps.
Amniotic membrane preparation
Freeze-dried human amniotic membrane tissue in its dry form is removed from its outer packaging but left in its inner packaging (foil on one side, clear plastic on the other). Using utility scissors, the AMT is cut through the packaging into a C-shaped graft (Figure 3) large enough to surround the conjunctival defect (Figure 4). This is placed to the side.
Fibrin adhesive preparation
The surgical assistant and circulating nurse prepare the fibrin adhesive as follows. The (scrubbed, gloved) surgical assistant holds a sterile 1 cc syringe with an 18-gauge needle and draws up about 0.1 cc of fibrinogen solution in a sterile fashion from the fibrin sealant vial (blue label), which is held inverted by the (not scrubbed) circulating nurse. Note the outside of the vial is not sterile, but the top can be wiped with alcohol to facilitate a sterile transfer to the surgical field. The same is done with the thrombin sealant (black label vial) using a separate 1 cc syringe and separate 18-gauge needle. The surgical assistant should be careful to include as little air as possible in the fibrinogen syringe. Next, into the thrombin-filled syringe the assistant draws up an additional 0.9 cc of balanced salt solution and inverts the syringe several times to mix the two. The adhesive components are now ready for use.

Amniotic membrane application
The bare sclera is now wetted with a few drops of balanced salt solution to allow the graft to hydrate and slide during the next steps. A small droplet of fibrinogen is placed on the surface of a Paton spatula. Using toothed forceps in one hand, the surgeon lifts the edge of conjunctiva to expose the potential space that was created around the bare sclera. This fibrinogen is then applied to the underside of the conjunctiva in the potential space (note no thrombin is applied at this point). This fibrinogen will help retain the AMT graft in the next steps.
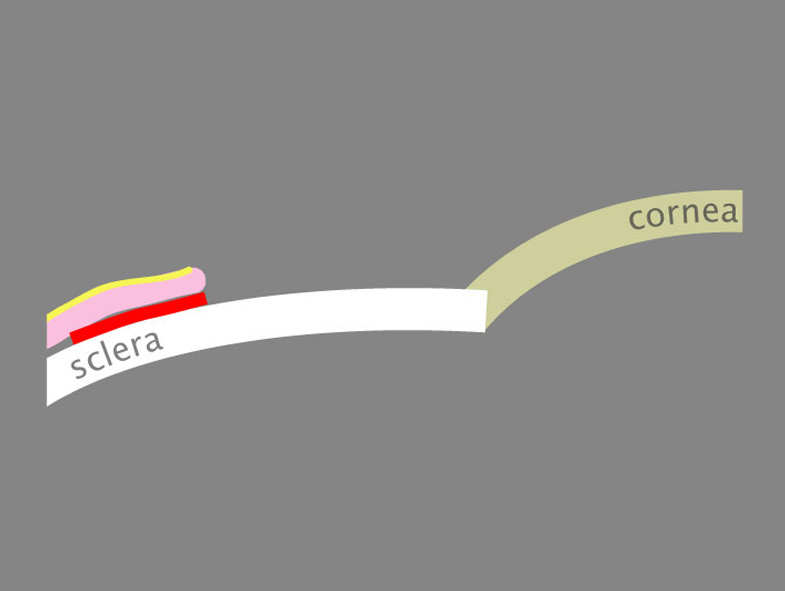
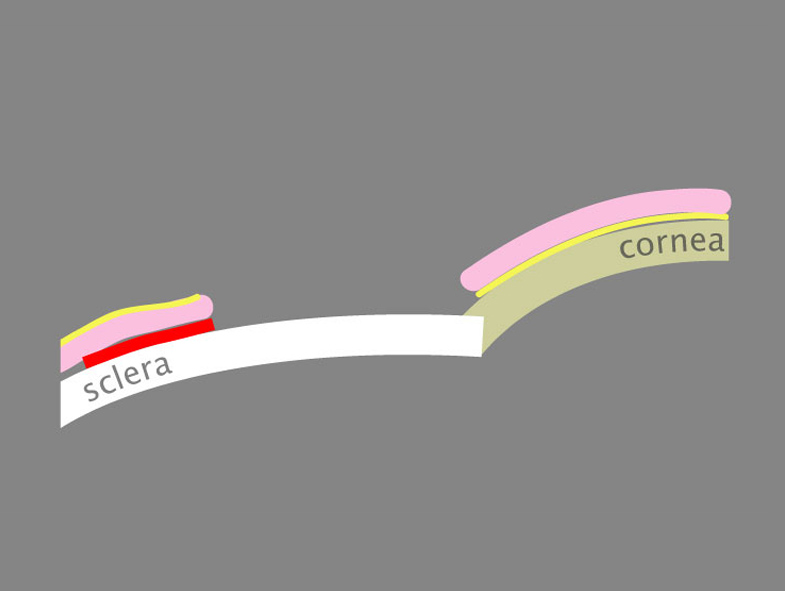
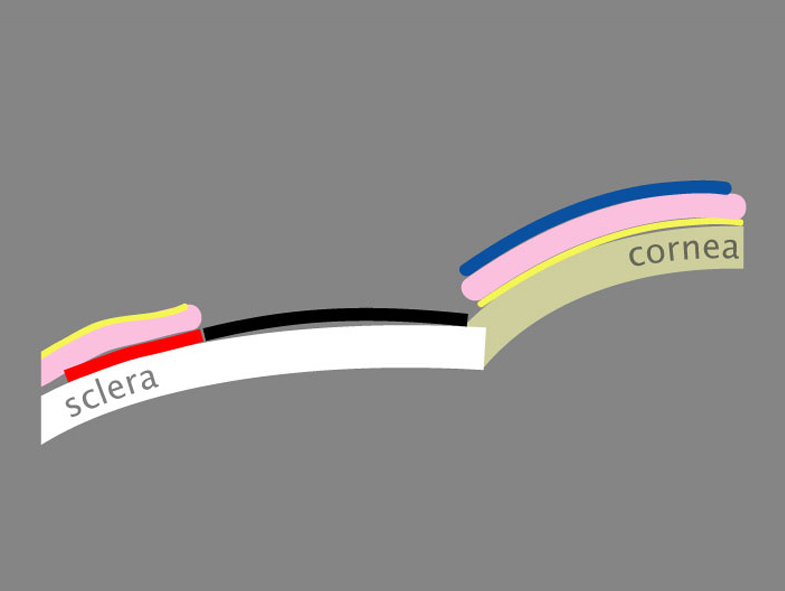
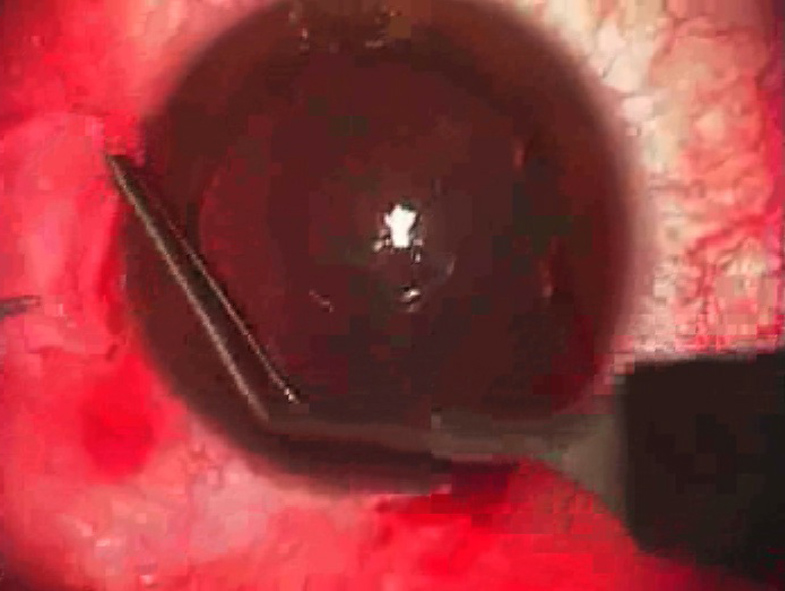
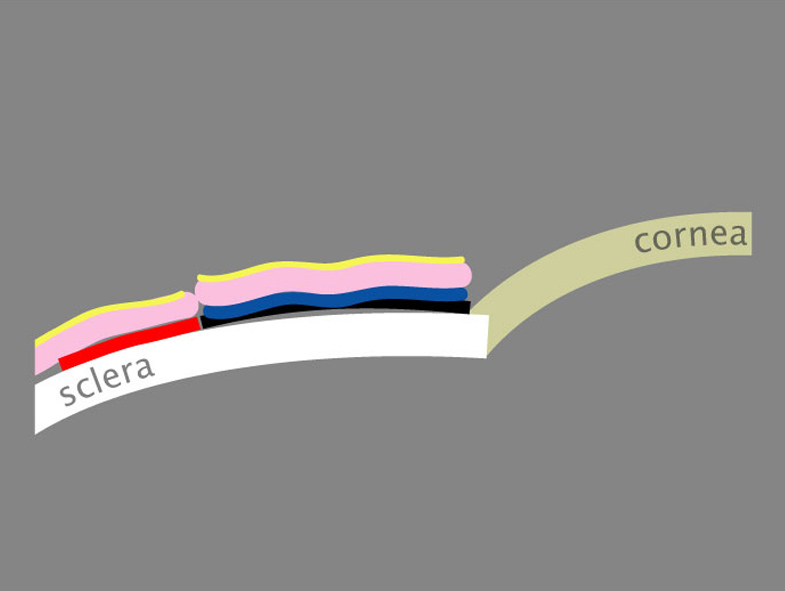
Attention is directed back to the amniotic membrane graft, which is removed from its packaging and placed on the bare sclera. Using toothed forceps, the surgeon lifts the conjunctiva to expose the potential space beneath it. At the same time, non-toothed forceps are used to grasp the edge of AMT and slide it from the bare sclera into the subconjunctival potential space (Figures 5 and 6). Care is taken to distribute the AMT evenly in this space, but some folds and turned corners of AMT are unavoidable and do not lead to problems after surgery. The surgeon’s goal is to create a “beltway” of AMT in the subconjunctival space around the excision site but not covering the bare sclera (Figure 7).
Once the AMT is in place, the surgeon can lift and advance the edges of surrounding conjunctiva toward the limbus to cover any remnants of AMT that are exposed. The presence of the fibrinogen, mixed with small amounts of thrombin in the patient’s own blood, will allow these edges to stay in place, covering all of the AMT.
Application of conjunctival autograft
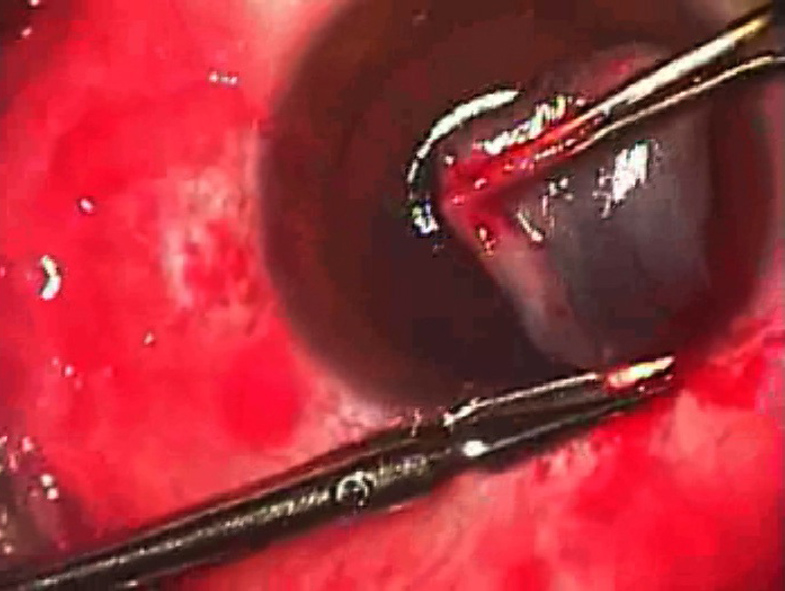
The conjunctival autograft, which remains attached to the superior limbus, is now reflected onto the cornea (epithelium to epithelium) and cut free from the superior limbus with scissors (Figure 8). The surgeon slides this graft across the cornea, orienting its limbal side to the limbus where the pterygium was removed (Figure 9). A small droplet from the diluted thrombin syringe (black label) is applied to the bare sclera (Figure 10), and a small droplet from the fibrinogen (blue label) syringe is applied to the underside of the graft (Figure 11). The graft is then grasped with two McPherson forceps and flipped onto the bare sclera site. This will mix the two components of adhesive, so the surgeon has approximately 30 seconds to “squeegee” the graft with the non-toothed forceps to orient it properly and approximate its edges with the edges of the surrounding conjunctiva and limbus (Figures 12 and 13). Once this is done, the surgeon should avoid unnecessary touching of the graft or surrounding conjunctiva, as this will only weaken the bonds of the fibrin adhesive. A fourth-generation fluoroquinolone is used q.i.d. for 1 week; prednisolone acetate 1% is used q.i.d. for 2 weeks and then tapered over 2 weeks; and bromfenac is used b.i.d. for 1 week.
Post-op follow-up/drug regimen
- Fluoroquinolone eyedrops (Zymar, Allergan, Irvine, Calif.) q.i.d. for 1 week.
- Prednisolone acetate 1% drops (Pred Forte, Allergan) q.i.d. for 2 weeks, then tapering off over 2 more weeks.
- Bromfenac (Xibrom, ISTA Pharmaceuticals, Irvine, Calif.) b.i.d. for 1 week.
- Return visit at 1 week.
Pearls
- Conservative use of cautery avoids post-op pain and is generally sufficient, as fibrin adhesive provides additional hemostasis.
- Dilution of one part thrombin with nine parts balanced salt solution slows down the polymerization process with fibrin adhesive and allows more time for manipulation of the graft.
- Harvesting a thin conjunctival autograft is best accomplished by making a small snip in the conjunctiva distal to the limbus, then lifting just the edge of conjunctiva (with minimal Tenon’s fascia) using toothed forceps. Blunt Wescott scissors can be inserted parallel to the conjunctival surface and then opened in the plane just below the conjunctiva to separate away most of Tenon’s.
- The conjunctival autograft should not be significantly oversized or contain excessive Tenon’s fascia, as these lead to excessive swelling after surgery.
- At follow-up a small amount of gap at the nasal edge of the graft may occasionally occur. This does not increase risk of recurrence.
Source (all): John A. Hovanesian, M.D.
References
- Kenyon, KR. Conjunctival Autograft Transplantation for Advanced and Recurrent Pterygium. Ophth 92:1461, 1985.
- Ma DH. Amniotic membrane graft for primary pterygium: comparison with conjunctival autograft and topical mitomycin C treatment. Br J Ophth 84:973, 2000.
- Hovanesian JA, Behesnilian A. Results of Pterygium Excision Using Amnionic Membrane Beneath the Healthy Conjunctiva Surrounding a Conjunctival Autograft. Poster at American Society of Cataract & Refractive Surgery Symposium. Chicago, 2008.
Editors’ note
Dr. Hovanesian is clinical assistant professor, Jules Stein Eye Institute, University of California, Los Angeles. He has no financial interests related to this article.
Contact information
Hovanesian: jhovanesian@harvardeye.com


