Glaucoma
Spring 2025
by Liz Hillman
Editorial Co-director
Pseudoexfoliation syndrome is a systemic, age-related disease—with an up to 20% prevalence in the 60+ age group—that most obviously affects the eye, though there is evidence that it has “associations … with cardiovascular and cerebrovascular morbidity” as well.1 These patients need more frequent monitoring due to an increased risk of developing secondary open angle glaucoma from the condition, and it can impact ocular surgery, such as cataract surgery, as well.
Kevin Halenda, MD, and Michael Krause, MD, PhD, provided their perspectives on the condition and advice for its identification, management, and considerations for surgery when pseudoexfoliation syndrome is present.
Prevalence and identification
Dr. Halenda said that pseudoexfoliation syndrome in his practice is not rare though not entirely common either.
“It’s probably under diagnosed. There are a lot of patients who have it, and there are some subtle exam findings,” he said.
“It’s probably under diagnosed. There are a lot of patients who have it, and there are some subtle exam findings.”
Kevin Halenda, MD
Dr. Krause has found in his diverse patient population that pseudoexfoliation is present in many different ethnic groups. The review by Schlötzer-Schrehardt and Naumann cited variation in prevalence with those of Nordic and Eastern Mediterranean descent being most affected. They stated that “variation in prevalence has been proposed to be due to epigenetics, the attitude of inhabitants, UV exposure, climatic conditions, proximity to the equator, dietary factors, oxidative stress mechanisms, genetic predisposition, etc.”1
Identification of pseudoexfoliation is important, Dr. Krause noted, because up to 40–50% of these patients will develop glaucoma as a result. As such, Dr. Halenda said if glaucoma is not yet present, he thinks patients with pseudoexfoliation should be seen in the clinic every 6 months. What’s more, he said glaucoma, if it develops, is often faster progressing and can be more severe.
“They tend to require surgery more frequently and earlier than in primary open angle glaucoma patients because they tend to present with more severe disease,” Dr. Halenda said, noting that he’ll often see patients who have been diagnosed with pseudoexfoliation glaucoma every 4 months until he has an idea of how stable their disease is.
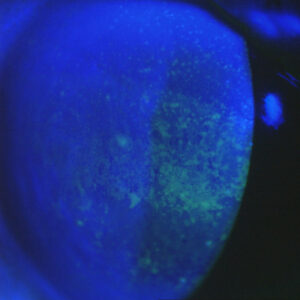
There are characteristic exam findings associated with pseudoexfoliation syndrome, Dr. Krause said, noting white fibrillar material on the iris border and white flaky deposits on the anterior capsule of the lens. He also said these patients typically dilate poorly, and there may be iris transillumination defects. On gonioscopy, the trabecular meshwork can be pigmented, and there may be a Sampaolesi line (pigment anterior to Schwalbe line).
In addition to these signs, Dr. Halenda said other clues include evidence of zonular instability such as one anterior chamber angle being narrower than the other.
If the patient has progressed to pseudoexfoliation glaucoma, Dr. Halenda said that it tends to be very asymmetric between eyes and presents with higher IOPs than those typically seen with primary open angle glaucoma.
“Sometimes the pressure can be very high, even higher than 50. One of the things that raises my suspicion for pseudoexfoliation glaucoma is if there is a big difference in the severity of the disease between the two eyes. It doesn’t mean that they have it, but it raises a red flag,” Dr. Halenda said.
Management
Dr. Krause said management with drops or SLT are both reasonable initial treatment strategies. Though, he noted, the effect of SLT may diminish more quickly in patients with pseudoexfoliation glaucoma.
“Since these patients often present with advanced damage, a surgical procedure is often necessary,” Dr. Krause added. “If possible, this should be combined with cataract surgery. Angle-based procedures like a goniotomy, Hydrus Microstent [Alcon], Omni [Sight Sciences], or iTrack Advance [Nova Eye Medical] are good minimally invasive options. However, filtration surgery with a XEN 45 Gel Stent [AbbVie], trabeculectomy, or glaucoma drainage implant may be required.”
Dr. Krause said that someday suprachoroidal shunts would be a welcome option to treat pseudoexfoliation glaucoma patients. Dr. Halenda said he prefers excisional procedures such as trabeculotomy or goniotomy when selecting MIGS for these patients.
Dr. Halenda said for all surgeries with this condition, patients can have more prolonged and profound inflammation. As such, they may require more aggressive and prolonged steroid tapers than typical.
Considerations for cataract surgery
There is a higher rate of complications for cataract surgery in patients with pseudoexfoliation syndrome, according to Dr. Halenda, primarily due to the effect of the condition on the zonules compromising lens stability.
He said it’s important to create a large enough capsulorhexis for these patients because they’re at higher risk for capsular phimosis later on, which could contribute to lens dislocation. He also said it’s important to minimize lens rotation, making sure there is adequate hydrodissection and potentially use of phaco-chop techniques.
Dr. Halenda said there is an increased risk of vitreous loss and zonular damage during cataract surgery in patients with pseudoexfoliation. In addition, the exfoliative material affecting the iris might necessitate use of a pupillary expansion ring or iris hooks. For lens instability, a capsular tension segment or capsular hooks might be needed.
“Some surgeons advocate for placing a 3-piece IOL in the capsule because it exerts a little more tension, which can increase stability,” he said. “Also, the exfoliative material does compromise the corneal endothelium, so they’re at greater risk for corneal decompensation after cataract surgery or any other intraocular surgery.”
Finally, Dr. Halenda said that these patients have a higher risk of IOP spikes after cataract surgery, especially if a MIGS procedure wasn’t performed. Thus, he said “it’s important to thoroughly irrigate the viscoelastic out of the eye after surgery.”
Article Sidebar
Lorraine Provencher, MD, EyeWorld Glaucoma Editorial Board member, shared what she is excited for at the ASCRS Annual Meeting:
“I love the ASCRS Annual Meeting! The content is highly relevant to anterior segment surgeons of all levels, but my favorite part is seeing all of my friends and colleagues.”
About the physicians
Kevin Halenda, MD
Assistant Professor of Ophthalmology
West Virginia University
Morgantown, West Virginia
Michael Krause, MD, PhD
Assistant Professor
University of Virginia
Charlottesville, Virginia
Reference
- Schlötzer-Schrehardt U, Naumann G. Ocular and systemic pseudoexfoliation syndrome. Am J Ophthalmol. 2006;141:921–937.
Relevant disclosures
Halenda: None
Krause: None
Contact
Halenda: kevin.halenda1@hsc.wvu.edu
Krause: XDB3ME@uvahealth.org