Cover Feature: Cornea
May 2008
by Vanessa Caceres
EyeWorld Contributing Editor
Some products are better than others for certain dry-eye conditions
Gels and ointments have their place to treat moderate and severe dry-eye patients, but they’re not without their challenges, say a number of physicians. First, not every gel or ointment is suited for every dry-eye patient, said Robert Latkany, M.D., founder and director, Dry Eye Clinic, New York Eye and Ear Infirmary, New York. “A lot of eye doctors are guilty of lumping all dry-eye patients together,” he said. In turn, they may recommend a gel or ointment not specific to the cause of the patient’s dry eye.
Additionally, gels and ointments are often misused by patients. Here are some red flags to avoid in your patients who use gels and ointments, followed by dry-eye gel and ointment recommendations for certain conditions.
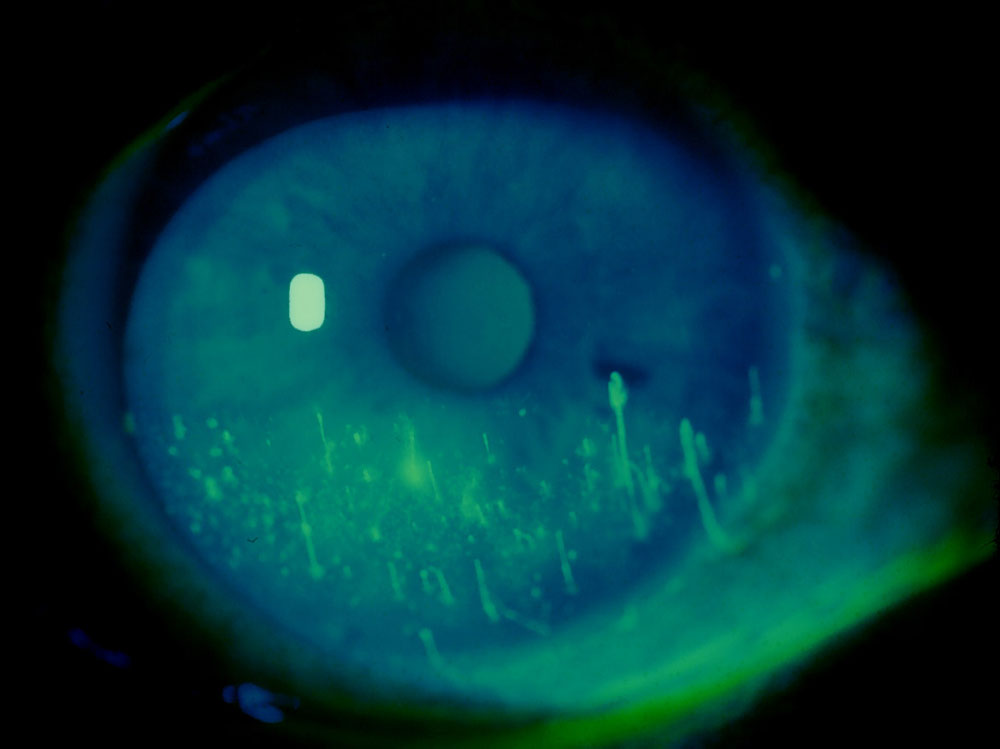
Source: Gary N. Foulks, M.D.
Misuses
Many physicians theorize that thicker gels and ointments can interfere with meibomian glands, actually making tear-duct problems related to dry eye worse. This is especially true in patients with meibomian gland disease, although it can occur in any dry-eye patient, said Gary N. Foulks, M.D., Arthur and Virginia Keeney professor of ophthalmology, University of Louisville, Ky. “Most of these ointments are relatively messy and not good at stabilizing the tear film—they may aggravate stability,” Dr. Foulks said. “They do provide mechanical protection to the eye, but I’m not usually recommending ointments for patients with meibomian gland disease.” This is especially true of petrolatum-based ointments, he added. Most of the ointments available are composed of petrolatum and mineral oil.
“Patients’ meibomian glands are clogged, and then they’re lathering ointment on them at night,” Dr. Latkany said. “Who’s to say what that does to those ducts? Does it make matters worse? My guess is yes.” So, the misuse often occurs when patients—or their eye doctors—recommend chronic use of an ointment without tracing the actual cause of the dry eye. “You can’t just throw ointment at them without any good direction and a sense of what could cause a problem,” Dr. Latkany said.
If a patient uses a gel or ointment daily for a long time, they may avoid discovery of the root cause of their dry eye—a situation that Rebecca Petris, founder, Dry Eye Company, Silverdale, Wash., has encountered frequently when she speaks with dry-eye patients.
“We routinely hear from patients who are kept on ointment nightly for a long time. They’ll say ‘It finally dawned on me that the longer I use this, the worse I feel,’” she said.
Another misuse is when patients do not practice good lid hygiene while using ointments, said Esen K. Akpek, M.D., associate professor of ophthalmology, and director, Ocular Surface Diseases and Dry Eye Clinic, Wilmer Eye Institute, Johns Hopkins University, Baltimore. She recommends that patients use the OCuSOFT scrub (Cyancon/OCuSOFT, Richmond, Texas) in tandem with ointment use. Otherwise, they can use hot compresses and scrub the lid and lid margins with diluted baby shampoo prior to ointment use.
Practitioners have to monitor for good lid hygiene along with the effectiveness of the gel or ointment, particularly in a patient with meibomian gland disease, Dr. Latkany said.
Sometimes patients can overuse gels and ointments or use them when they don’t actually need them. “For mild dryness, very thick gels and ointments are often not necessary,” said Roy S. Chuck, M.D., Ph.D., Tom Clancy Professorship in Ophthalmology, and director of refractive surgery, Wilmer Eye Institute, Johns Hopkins University.
“A thinner drop applied more frequently which does not blur vision would be adequate in these cases. Of course there is also the problem of too frequent application of artificial tears as well,” Dr. Chuck said.
Occasionally patients will use the more viscous ointments during the day, when they’re actually meant for nighttime use only, Dr. Akpek said.
What works best
Gels, which usually are not as thick as ointments, can be used by patients with mild to moderate dry eye, physicians said. It is common to recommend them to patients who wake up in the morning with dry eye, Dr. Chuck said. GenTeal Gel (Novartis, Basel Switzerland) is a well-liked gel for Dr. Akpek’s patients. Ointments often are used by patients with lagophthalmos, Dr. Latkany said. Although older studies estimate that 4% of the population has lagophthalmos, his own estimates are actually closer to 15% to 20%. Ointments—preferably preservative-free ones—help patients with ocular surface disease protect their eyes while sleeping. “Sleeping is important because it allows them to recover and bathe and restore the eye’s good health,” he said.
“If patients use their gels or ointments before bedtime, I ask them to use something very thick that will blur their vision, such as Lacrilube [Allergan, Irvine, Calif.] or Celluvisc [Allergan],” Dr. Chuck said.
Another option to use instead of or along with an ointment is a goggle created for use in dry-eye patients. The Tranquileyes goggle (eye eco, Temecula, Calif.) has foam pads inside of them that help humidify the eye while the person is sleeping. “There’s a role for these goggles,” said Dr. Latkany, adding that a few patients feel claustrophobic in them or experience an allergic reaction to the foam pads.
Dr. Akpek also likes the use of special goggles for lagophthalmos patients and patients with sleep apnea who use a C-PAP machine and in turn have floppy eyelid syndrome. However, she’ll recommend use of the goggles along with an ointment.
Patients can also tape their lids at night with hypoallergenic paper tape found at pharmacies, Dr. Latkany said. Dr. Akpek favors this approach as well but usually prefers it only for unilateral problems—taping of both eyes could increase the risk for falls, especially in elderly patients.
If all options to help nighttime dry eye fail, Dr. Foulks will look at surgical options. “If patients have significant lagophthalmos that we can’t control, I’ll usually ask the plastic surgeon to look at them to see if they can fix the eyelid,” he said.
Patients with recurrent corneal erosions frequently use a hypertonic ointment at night, such as Muro 128 (Bausch & Lomb, Rochester, N.Y.). “It draws water out of the epithelium,” Dr. Akpek said.
Dr. Foulks said that another option for patients with epithelial edema is a drop called Dwelle, which is sold through the Dry Eye Company. Made of polyvinyl alcohol 2.7% and povidone 2% and manufactured as a dry-eye lubricant, it was developed by Frank J. Holly, Ph.D., Yantis, Texas.
“Dwelle has colloidal osmolarity that is slightly hypertonic to the corneal swelling pressure. It will pull fluid from the corneal epithelial cells and hold it on the surface. I found that to be quite effective,” Dr. Foulks said. He has found that Dwelle can help patients with epithelial edema, recurrent corneal erosions, and even diabetic keratopathy.
Editors’ note
Drs. Latkany, Foulks, and Akpek have no financial interests related to their comments. Ms. Petris’s company, Dry Eye Company (Silverdale, Wash.), distributes Dwelle drops and Tranquileyes goggles. Dr. Chuck has financial interests with Alcon (Fort Worth, Texas) and Allergan (Irvine, Calif.).
Contact Information
Akpek: 410-955-5494, esakpek@jhmi.edu
Chuck: 410-583-2802, rchuck1@jhmi.edu
Foulks: 502-852-6150, gnfoul01@gwise.louisville.edu
Latkany: 212-832-2020, relief@dryeyedoctor.com
Petris: 877-693-7939, ext. 717, rebecca@dryeyecompany.com



