Glaucoma: Glaucoma fundamentals
August 2016
by Stefanie Petrou Binder, MD,
EyeWorld Contributing Writer

The nomenclature of angle closure has undergone an important shift in the past few years, and a familiarity with this nomenclature and the management of various manifestations of angle closure is very important for all ophthalmologists to understand. A “primary angle closure suspect” is a patient with narrow angles who does not have any other concerning findings on exam: i.e., no peripheral anterior synechiae (PAS), no elevated intraocular pressure (IOP), and no glaucomatous optic neuropathy (GON). The term “primary angle closure” is reserved for a patient with narrow angles who has either PAS or elevated IOP or both but does not have GON. The term “primary angle closure glaucoma” is reserved for patients with narrow angles, PAS or elevated IOP, and GON. In this month’s “Glaucoma fundamentals” column, we address the management of the primary angle closure suspect. The mainstay of treatment for the primary angle closure suspect is laser peripheral iridotomy (LPI). However, how these patients should be managed and followed after LPI is done is not always well understood, particularly if the LPI does not effectively open the angle. To answer the question of “What do I do if the LPI does not open the angle?” we sought the opinions of 2 glaucoma specialists: Edward Barnett, MD, and Shan Lin, MD.
—Husam Ansari, MD, Glaucoma fundamentals editor
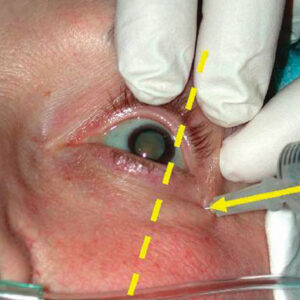
Is an angle closure glaucoma suspect off the hook once the laser peripheral iridotomy (LPI) is performed? Not quite

Source: Shan Lin, MD
Laser peripheral iridotomy (LPI) is used in primary closed angle suspects to reduce the risk of potentially severe and visually traumatic angle closure attacks. LPI allows improved flow of aqueous humor between the anterior and posterior chambers, and helps prevent the slow formation of sub-acute closed angle glaucoma. Primary angle closure can come about in eyes in which certain anatomic conditions, such as a short eye, hyperopia, or a growing cataract, gradually narrow the chamber angle over time. Although not all patients with narrow angles go on to develop angle closure glaucoma, laser iridotomy is performed because of its relatively low risks compared to the more serious consequences of angle closure glaucoma. For primary angle closure suspects, LPI is currently the preferred method of treatment. But whether the iridotomy treatment opens the angle or not, physicians need to keep an eye on anyone who has, or had, narrow angles.
Angles that open
Even when an iridotomy improves the angle in a primary angle closure suspect, specialists say that it is still important to continue to follow these patients over time. According to Edward Barnett, MD, PhD, professor of ophthalmology, Medical College of Wisconsin, Milwaukee, the frequency of follow-up visits depends on patient characteristics. “If the patient does not have a high-risk finding such as high hyperopia, anterior uveitis, or a large, mature cataract, then I typically recommend an annual exam, which includes pre-dilation gonioscopy,” he said. Patients in whom past intermittent angle closure is suspected warrant closer follow-up even if the angle improves following LPI, as any episode of appositional closure may damage the trabecular meshwork and increase the risk of future “residual” glaucoma. “If the patient’s angle is open after the LPI but still shows a definite plateau iris configuration, I would routinely check the eye pressure following dilation to evaluate the risk of future plateau iris syndrome. Gonioscopy and anterior segment imaging both before and after pilocarpine in the office can be useful in confirming a plateau iris,” Dr. Barnett said.
He explained that dilation can be a concern in individuals who need to have their eyes dilated frequently, such as patients with exudative macular degeneration or diabetic retinopathy. “Even if these patients had an LPI performed, I will generally make sure that the pressure does not become elevated in the office following dilation. Of course patients can still go on to have an angle closure event after leaving the office, as the pupil comes down in size over the next several hours, so careful patient instruction on the symptoms of acute angle closure remains important.”
Angles that stay occludable
When iridotomy leaves the angle narrow and occludable in a primary angle closure suspect, the physician may need to act to reduce the risk of future angle closure. Treatment, as always, is decided case by case. “If patients remain narrow after LPI, I will observe them more closely over time with repeated gonioscopy and also anterior segment ultrasound or OCT to identify less common causes of angle closure. If the patient is older and has visually significant cataract, I may recommend proceeding with cataract surgery, which generally improves the angle,” Dr. Barnett said. Even in younger patients, clear lens extraction may rarely be indicated in some cases such as nanophthalmos or in patients with extremely narrow angles and a history of angle closure in the fellow eye. Another treatment Dr. Barnett implements in patients with occludable angles after LPI is iridoplasty. He explained, “I will typically perform iridoplasty in those rare patients who have demonstrated plateau iris syndrome with elevated IOP and less commonly as a preventative measure in patients with extremely narrow angles and early PAS formation.”
Shan Lin, MD, professor of clinical ophthalmology and director of the glaucoma service, Department of Ophthalmology, University of California, San Francisco, thinks that iridoplasty, while often effective, is somewhat controversial. “I think that there needs to be more good studies that are prospective and randomized to detail whether iridoplasty is really of benefit to the patient in the long term. There are doctors who feel strongly about giving their patients argon laser iridoplasty and others, like myself, who feel that it is thus far unproven. There are potential side effects related to using argon laser iridoplasty, and in my experience I don’t see the necessary benefits.” Dr. Lin added, “I transitioned from someone who frequently did this procedure to someone who usually observes these cases.”
Iridoplasty creates burns at the peripheral iris using an argon laser to shrink the iris and pull it away from the chamber angle and open it up. Dr. Lin takes a conservative approach to iridoplasty but thinks it may be warranted in some cases. He said, “The procedure is reasonable in patients who are very narrow in which all 4 quadrants look occludable—grade 1 or grade 0—and where there is a very high risk for an attack of glaucoma or closure despite the iridotomy. In those patients I’d consider iridoplasty. Another category would be people who are progressing and developing PAS, which pushes them into primary angle closure status. I would consider iridoplasty here to prevent them from progressing.”
Dr. Lin uses the argon laser starting at 200 mW at 0.5 s duration. He places roughly 30 500 µ spots around the peripheral iris, placing them as far into the periphery as possible. Postop care focuses on reducing inflammation and is carried out using 4x daily prednisolone drops for 3 to 7 days.
Dr. Lin explained that iridoplasty is, unfortunately, not foolproof. “Failure of iridoplasty, in my experience, has been in patients, for example, who have plateau iris or who have a large lens that pushes everything forward, in whom the angle remains narrow.”
Narrow angle detection
When a patient visits him for the first time or for a follow-up visit, Dr. Lin uses slit lamp and gonioscopic examinations to rule out narrow chamber angles. If he suspects a narrow angle, he will then use anterior segment OCT, which he repeats on a routine annual basis in closed angle suspects for a true, objective assessment of the angle. He said, “Gonioscopy is revealing, but it requires skill and experience, since it’s an indirect way of looking at the angle. Ultrasound biomicroscopy is also very helpful, for instance, if I do an iridotomy and the angle remains narrow and I want to understand the mechanism why. Its drawbacks include that it is a contact procedure, which is losing a little favor in the U.S. these days, and that you need an ultrasound specialist,” he explained.
Editors’ note
Drs. Barnett and Lin have no financial interests related to their comments.
Contact information
Barnett: ebarnett@mcw.edu
Lin: shan.lin@ucsf.edu