October 2017
Cover Feature: Challenging cataract cases
by Ellen Stodola
EyeWorld Senior Staff Writer
Diabetic patients should be identified and managed prior to cataract surgery
When preparing for cataract surgery, ophthalmologists have to consider a variety of factors, including other diseases and comorbidities. A patient with diabetes may require special considerations, and a careful examination prior to surgery should be performed. It may be helpful to have a retina specialist involved.
David Boyer, MD, Retina-Vitreous Associates Medical Group, Los Angeles, Bonnie Henderson, MD, Ophthalmic Consultants of Boston, Boston, Keith Warren, MD, Warren Retina Associates, Overland Park, Kansas, and Walter Stark, MD, retired professor of ophthalmology, Johns Hopkins University, Baltimore, weighed in on the diabetic patient presenting for cataract surgeon, how the cataract and/or retina surgeon should proceed, which medications may be helpful, and other factors for a successful surgery.
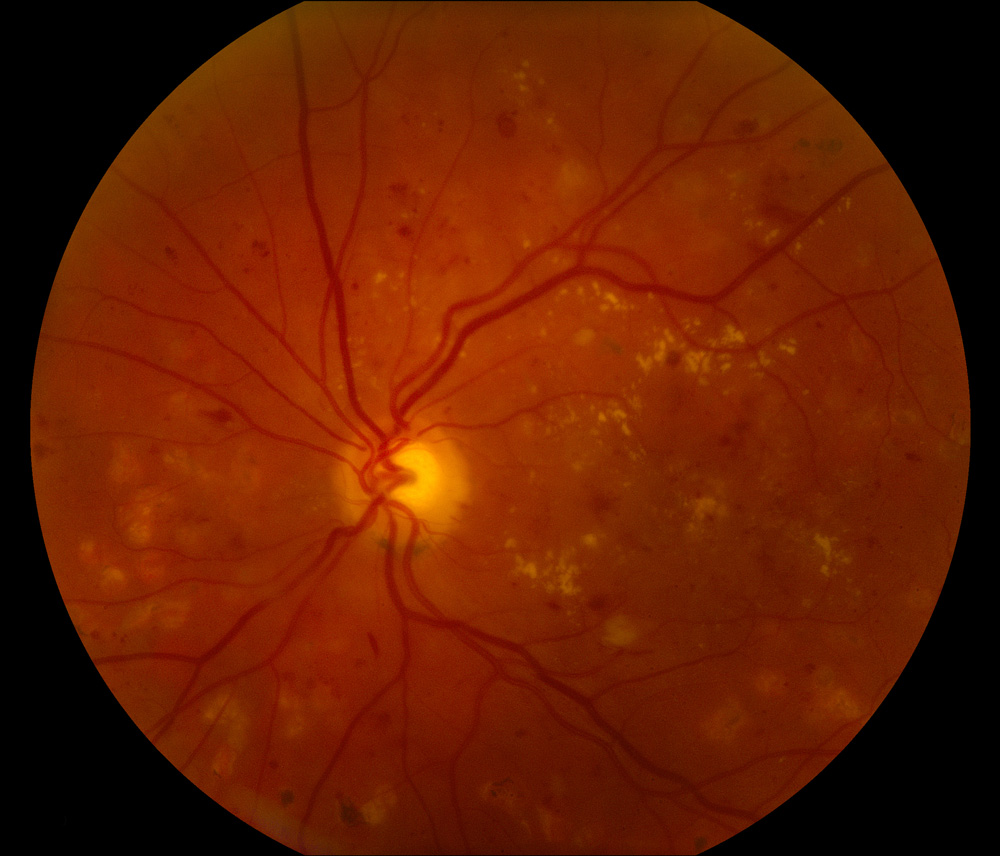

Source (all): Keith Warren, MD
Evaluating a diabetic patient
Dr. Boyer said the age of the patient, control of diabetes, and presence of diabetic retinopathy all need to be evaluated to help determine what lens is most appropriate. “If the patient has tractional detachment or appears he or she may need vitrectomy surgery in the future, the cataract surgeon should avoid silicone lenses and hydrophilic lenses,” he said. “If there is macular edema, multifocal lenses should not be used.” He added that preoperative OCT, OCTA, and wide field fluorescein may be indicated.
Dr. Henderson recommended performing a macular OCT on every diabetic patient. It is often difficult to assess the macula with a visually significant cataract. Knowing the status of the macula before surgery becomes even more important when there is an increased risk of developing postoperative macular edema. “There have been many times when the macula appeared normal on the slit lamp exam but the OCT revealed subtle underlying pathology,” Dr. Henderson said. “This allowed me to counsel the patient appropriately and refer to a retina specialist if needed.”
Diabetes and cataract are common, Dr. Warren said, adding that the literature states that about 15% of patients undergoing cataract surgery will have diabetes. Diabetes is a disease that affects blood vessels and surgery causes inflammation of blood vessels, so if you have both active at the same time, this could lead to a bad outcome, Dr. Warren said. The cataract surgeon should have a good idea about the status of the patient’s diabetes, if retinopathy is present, and if he or she has edema. “The cataract surgeon needs to evaluate patients for the presence of retinopathy before surgery,” he said. This evaluation should include a careful slit lamp exam and evaluation of the retina. Additionally, those patients would most likely benefit from obtaining OCT prior to surgery to determine if any edema is present in the retina.
In patients with diabetes but no retinopathy, retinal edema may occur following cataract surgery, and if the patient has retinopathy and macular edema prior to surgery, this is likely to get worse.
It’s important in managing patients to evaluate them for the presence of retinopathy, Dr. Warren said, and if they have it, warn them that even with perfect cataract surgery, they are not likely to have perfect vision following the surgery.
“Diabetic patients are more prone to a variety of complications,” Dr. Stark said. “If they already have diabetic retinopathy or some macular edema, visual acuity is not going to be restored to 20/20, so one has to set realistic expectations about the outcome.” Diabetes can affect almost all areas of the eye, including increasing the risk of cataract formation, causing problems with the corneal epithelium, and causing neovascularization of the iris. “It’s important that a thorough retinal exam be done pre- and postoperatively, including OCT,” he said.
Retina specialist’s role
Preop OCT, OCTA, and wide field fluorescein angiography may be needed to evaluate the patient preop, Dr. Boyer said. “The retinal surgeon should evaluate the diabetic status and dry the macula up to minimize edema from worsening.”
A patient undergoing active treatment for macular edema may need an injection 1–2 weeks before surgery, he added. “The patient with severe vascular non-perfusion may require panretinal photocoagulation prior to surgery,” Dr. Boyer said. “Certainly the patient needs to be followed carefully for the formation of rubeosis or vitreous hemorrhage.”
NSAIDs and management of diabetic patients
Studies have shown an improvement in CME with patients on NSAIDs, Dr. Boyer said, and he recommends they be started 1–2 weeks before surgery and continued 5–6 weeks after. “I recommend they be used even if no retinopathy is present,” he said. “Postop uncomplicated cataract surgery still has a slight increase in thickening on OCT, though the vision isn’t altered.”
Dr. Warren said physicians must consider different patient types: those with diabetes but no retinopathy, those with retinopathy and no edema, and those who have both retinopathy and edema. For patients with diabetes with no retinopathy, consider 6 weeks of postop anti-inflammatory medication. Patients with diabetes and retinopathy but no edema have a higher risk of developing swelling and edema and should be treated for 6 weeks with anti-inflammatory therapy and should have the macula monitored at 1 week and 1 month postop. Finally, patients with diabetic retinopathy and macular edema should have surgery deferred until they have had treatment for the macular edema, which means at least three injections of anti-VEGF therapy and no active edema before surgery. If the edema is chronic, Dr. Warren said, they should consider a depot steroid injection prior to surgery, and they should be managed with OCT and be advised that the outcome may be guarded.
The use of NSAIDs can be controversial, Dr. Henderson said. According to the ASCRS Clinical Survey, the majority of ophthalmologists in the U.S. and worldwide use NSAIDs preop and postop for high risk patients, such as diabetics. Most start NSAIDs 3 days prior to surgery and will continue for 1–3 months even after uncomplicated surgery for diabetics.
“Many peer-reviewed studies have shown that using NSAIDs perioperatively can be beneficial in decreasing the risk of developing and treating macular edema,” Dr. Henderson said. “I prescribe topical NSAIDs for all diabetics for 3 months after cataract surgery.”
Multifocal IOLs in patients with diabetic retinopathy
Dr. Boyer does not think that a multifocal lens is a good choice for these patients. An OCTA may aid in determining the status of the macula, he said.
With multifocal IOLs, one loses about 20% of overall quality of vision, Dr. Stark said, and patients put up with that to see at distance and near. “But when you’re dealing with a diseased eye, I don’t think it’s a good idea to put in a multifocal IOL,” he said.
Multifocal IOLs can decrease contrast sensitivity, Dr. Henderson said, so it is important to assess the eye carefully for other comorbid diseases. “If a patient has significant diabetic retinopathy, I usually do not recommend a multifocal IOL,” she said. “If the amount of retinopathy is mild, stable, and there is no macular disease, it is reasonable to discuss multifocal IOLs.” The preoperative counseling is crucial to discuss the potential disadvantages and limitations of multifocal IOLs, Dr. Henderson added.
Dr. Warren does not think a multifocal lens is an appropriate option for a patient with diabetes and shouldn’t be used at all if the patient has retinopathy. He said that 95% of patients who have diabetes more than 20 years will have some form of retinopathy. Multifocals reduce contrast, Dr. Warren said, so they are not a good option for a diabetic, and if the patient already has edema, this also reduces contrast.
Postop CME in diabetic eyes
If a patient develops CME, regardless of a history of diabetes, Dr. Henderson obtains the advice of her retina colleague. “I will usually start with topical steroids and NSAIDs,” she said. “If the edema persists, other options such as injections of steroids or anti-VEGF agents are considered depending on the patient.”
The rate of postop macular edema would be greater in these patients, Dr. Stark said, adding that the ophthalmologist would want to cut down on inflammation as much as possible. Preop and postop NSAIDs can be used but that physicians should be careful if the patient has a persistent epithelial defect.
Dr. Boyer usually starts with topical drops—steroid and non-steroidal—but moves to intravitreal steroid injections if no progress is seen when patients are treated.
Editors’ note
Drs. Boyer, Henderson, Stark, and Warren have no financial interests related to their comments.
Contact information
Boyer: vitdoc@aol.com
Henderson: bahenderson@eyeboston.com
Stark: wstark@jhmi.edu
Warren: kwarren@warrenretina.com

