Cover Feature: Corneal infections
February 2014
by Michelle Dalton
EyeWorld Contributing Writer
A new retrospective analysis suggests oral azithromycin may be beneficial
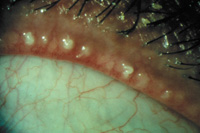
Source: John D. Sheppard, MD
According to the recent International Workshop on Meibomian Gland Dysfunction (MGD), “terms such as ‘meibomitis’ or ‘meibomianitis’ describe a subset of disorders of MGD associated with inflammation of the meibomian glands,” but inflammation is not always associated with MGD and therefore, the terms are not interchangeable.1
Further, the etiology of meibomitis “has not been fully sorted out,” said Todd P. Margolis, MD, professor of ophthalmology, Washington University, St. Louis, adding there may be an inflammatory aspect within the lipids.
An issue for clinicians is simply the definition of meibomitis, and there has yet to be a universally accepted method on how to describe it—or how to treat it, said Joseph Tauber, MD, in private practice, Kansas City, Mo.
MGD itself is generally recognized as a common disease and one of the most common causes of dry eye disease, said Michael Lemp, MD, clinical professor of ophthalmology, Georgetown University, Washington, D.C., and chief medical officer, TearLab Corp., San Diego. “But we have to consider what causes it. Is it an infectious disease? What role does inflammation play? We still do not have all the answers.” If MGD persists for a long enough time, it will stimulate inflammatory activity in the lacrimal glands, he said.
Azithromycin is a macrolide antibiotic that also has anti-inflammatory properties, Dr. Margolis said. In its topical form, the compound is approved for the treatment of bacterial conjunctivitis and has been studied for the treatment of blepharitis.
“There was some logic behind evaluating the oral version of azithromycin for lid disorders,” Dr. Margolis said, who, with colleagues, retrospectively evaluated oral azithromycin in patients with refractory meibomitis, dosed at 1 g orally once a week for three weeks.2 The analysis found about 70% of the patients had improved symptoms.
With no real guidelines on how to uniformly define or evaluate these disorders, “we’re in unchartered waters in how to be objective,” Dr. Tauber said. “It’s not unusual to hear that someone is using oral azithromycin in some of these refractory cases.”
Using a systemic drug to treat an ocular disorder has potential, but physicians should still start with the established care routines that include lid massage, lid hygiene, and topical antibiotics, said James McCulley, MD, chair of ophthalmology, UT Southwestern Medical Center, Dallas.
“If a patient fails standard therapy, then I’d consider oral azithromycin,” Dr. McCulley said, who added the study has “thrown out an interesting thought, but there’s no good data to support the hypothesis. It’s objectively weak support for oral azithromycin; most clinicians should read the study and come to the reasonable conclusion that the findings are interesting, but not that they should overhaul their current treatment regimens.”
Agreed Gary Foulks, MD, emeritus professor of ophthalmology, University of Louisville School of Medicine: “The study remarks only on improvement in symptoms and not the objective features of MGD. I believe topical azithromycin works, but I suspect oral azithromycin also would work.” Dr. Foulks added that the American Academy of Ophthalmology guidelines on blepharitis “carry a strong warning about use of oral azithromycin due to cardiac deaths reported with its use for other conditions.”
Role of oral azithromycin in ocular surface disorders
“As clinicians, we can’t be against any potential treatment,” Dr. Lemp said. “This analysis gets into one of the issues about ensuring what it is you’re treating. Is there a difference between meibomitis and MGD?”
The original intent of the retrospective study (n=32) was to show possible evidence that oral azithromycin may be a useful adjunct in patients who were not responding to other treatments, said Bennie H. Jeng, MD, professor and chair, Department of Ophthalmology and Visual Sciences, University of Maryland School of Medicine, Baltimore, and one of the co-authors of the analysis.
“When we looked at patients who had failed previous topical therapy—antibiotics, steroids, or some combination—they still improved after oral azithromycin,” Dr. Jeng said.
Patients were receiving three weeks of azithromycin at therapeutic levels, Dr. Margolis said, ensuring that any bacterial component would be eradicated.
“Patients were coming in saying they felt better. It was irrelevant what the previous treatments had been—on oral azithromycin and a topical agent for the lid margins, we achieved tremendous success rates,” he said.
Dr. McCulley said the finding is “something short of a proof of concept, but it is a very interesting thought and results are preliminary,” mainly because the analysis was not controlled and there were no details on what, if any, standard previous failed therapies had been.
“The benefits reported were only for a few weeks,” Dr. McCulley said. “It’s an interesting observation that needs further investigation in an appropriately controlled clinical trial.”
Oral azithromycin should “absolutely” be considered as a potential treatment for meibomitis, Dr. Tauber said, as the compound has both anti-inflammatory and antimicrobial properties.
Dr. Jeng said the analysis elucidated the long-lasting effects of azithromycin, although he continues to recommend initiating treatment with lid hygiene (e.g., mechanical scrubbing).
“Once failure happens with conservative treatment, then I used to invoke tetracycline derivatives,” he said, primarily doxycycline. “But that has to be taken twice daily for an extended period of time; oral azithromycin is dosed once a week for three weeks. The catch, of course, is the potential for it to create irregularities in heart rhythm.”
There has been some clinical efficacy with pulsed dosing of oral azithromycin in the treatment of posterior blepharitis,3 with all clinical outcomes and most subjective symptoms statistically improved after the 500 mg/day for three days in three cycles with seven-day intervals were implemented.
“Other smaller studies have been mentioned in some of the peer review as well,” Dr. Tauber said. “But there’s been no standardization in the treatment dosing, so it remains unknown what the best course may be.”
Current treatment strategies
In treating patients who have been unsuccessfully managed previously, “if they have failed topical azithromycin therapy, I will move to more intense lid expression, continued doxycycline use, topical cyclosporine, and possible LipiFlow therapy,” Dr. Foulks said, noting he has not yet used oral azithromycin in refractory patients.
Dr. Tauber said when patients are referred to him who have not achieved the comfort they need, “you have to go back to the beginning and start over. Lid hygiene is downright essential.” He recommends using a gel mask that can be microwaved to make it easier to achieve heated lid expression.
Dr. McCulley is an advocate of both doxycycline and minocycline (in Texas, many of his dermatologist colleagues prefer minocycline over doxycycline, so he tends to prescribe the former more often).
“People who prefer using doxycycline cite that minocycline may cause tinnitus in some patients,” he said, but added studies have shown minocycline “penetrates the tissue much better than we anticipated, well enough to eradicate Staphylococcus aureus.”4 Dermatologists cite the tetracycline derivative’s therapeutic benefit in acne rosacea as well, he said.
“Doxycycline has been used for more than 30 years,” Dr. Margolis said. “Some patients respond, some don’t. Clinicians need to ask what their ultimate end point is—do you want your patients to have ‘less red’ or do you want them to walk out of your offices feeling better? My focus has always been on comfort.”
Any of the oral tetracyclines have “justifiably earned a place in the treatment of meibomitis, MGD, and rosacea,” Dr. Foulks said. “We demonstrated improvement in the character of the lipid secretion with oral doxycycline, but it took longer than topical azithromycin and resulted in different changes in the lipid than occur with topical azithromycin.”5
When clinicians are treating lid disease and patients feel better, Dr. Lemp cautions the ocular surface may still be unhealthy and to be vigilant in treating any surface disorders as well.
Dr. Margolis said he advocates ascertaining the “real problem” for these patients.
“Horrible pain post-LASIK is not the same as a chronic surface or lid disorder that’s causing pain,” he said. “If there’s some degree of MGD and the patient complains of pain, we’ll likely start them on steroids, follow for about four weeks and re-evaluate, with the caveat that if the patient experiences any side effects to stop treatment and come in immediately.”
Doxycycline can lead to yeast infections and upset stomach in addition to skin disorders; Dr. Margolis has not seen the same types of reactions with oral azithromycin. He disagrees with intensifying lid hygiene, however.
“The more you manipulate the lids, the more you’re going to irritate them,” he said. “I take a more minimalist approach and recommend the patient rub a little steroid into the lids at the outer edges only once or twice a day.” Patients seem to appreciate that they are applying a mild steroid to the lid margins only, Dr. Margolis said.
Dr. Jeng said while results of the current analysis are far from perfect, “what I’m hoping is that people will start thinking about oral azithromycin. And maybe that can lead to a prospective trial on the treatment.”
References
- Nelson JD, Shimazaki J, Benitez-del-Castillo J, et al. The International Workshop on Meibomian Gland Dysfunction: Report of the Definition and Classification Subcommittee. Invest Ophthalmol Vis Sci. 2011;52(4): 1930–1937.
- Greene JB, Jeng BH, Fintelmann RE, Margolis TP. Oral azithromycin for the treatment of meibomitis. JAMA Ophthalmol.doi:10.1001/jamaophthalmol.2013.5295 Published online Nov. 7, 2013.
- 3. Igami TZ, Holzchuh R, Osaki TH, Santo RM, Kara-Jose N, Hida RY. Oral azithromycin for treatment of posterior blepharitis. Cornea. 2011;30(10):1145-9.
- Ta CN, Shine WE, McCulley JP, Pandya A, Trattler W, Norbury JW. Effects of minocycline on the ocular flora of patients with acne rosacea or seborrheic blepharitis. Cornea. 2003;22:545-548.
- Foulks GN, Borchman D, Yappert M, Kakar S. Topical Azithromycin and Oral Doxycycline Therapy of Meibomian Gland Dysfunction: A comparative clinical and spectroscopic pilot study. Cornea. 2013;32:44-53.
Editors’ note
The physicians have no financial interests directly related to their comments, although they have all conducted research on the topic.
Contact information
Foulks: foulksgary@gmail.com
Jeng: bjeng@som.umaryland.edu
Lemp: malemp@lempdc.com
Margolis: todd.margolis@ucsf.edu
McCulley: james.mcculley@utsouthwestern.edu
Tauber: jt@taubereye.com


