ONLINE EXCLUSIVE
ASCRS News
May 2026
by Liz Hillman
Editorial Co-Director
The first robot-assisted cataract surgery was accomplished just a few months ago, ushering in a new age of anterior segment surgery. A symposium at the 2026 ASCRS Annual Meeting—“Robotic Surgery: How Soon and How Good Will It Be?”—gave an overview of robotic cataract surgery and its future with perspectives from physicians who were directly involved with these rapidly advancing technologies.

Source: ASCRS
Session moderator John Hovanesian, MD, said in the future, robotic ophthalmic surgery will be designed to increase safety, efficiency, and precision. He predicted that patient demand and surgeon enthusiasm will influence the direction and adoption of robotic cataract surgery, but he added that surgeons will need to see real value of such systems before they become mainstream.
Dr. Hovanesian listed several companies working on robotic ophthalmic surgery, both within the anterior and posterior segment. One of the challenges these systems face, he presented, is what they are going to do in the real world with real patient variables, such as unexpected patient movement. “We need machines that can similarly [to human surgeons] protect patient safety,” he said.

Source: ASCRS
Neda Shamie, MD, discussed a “pre-robotics” topic, specifically the ALLY Adaptive Cataract Treatment System (LENSAR). She described the technology as a “stepping stone” in robotics, calling it “an inflection point in cataract surgery practice.” She went on to describe how the system has changed her approach to patient care.
“The preop device integration … has been a game changer for me. It’s seamless data integration,” she said. “The AI-guided imaging allows me to become a better surgeon.” The system’s iris registration has been helpful as well. “No longer do I have to worry about cyclotorsion and marking. Iris registration and its compensation for cyclotorsion has been an incredible addition to the way I treat patients, whether it’s LRIs or toric IOL alignment. It has minimized my need for intraoperative aberrometry, and it has improved my efficiency.”
Going back to data integration, Dr. Shamie said that future robotic systems should allow for surgeons to use the diagnostic tools they prefer. “It cannot be that it is married to one diagnostic device,” she said, explaining how ALLY brings in data from multiple diagnostic tools, enhancing precision, efficacy, and consistency.
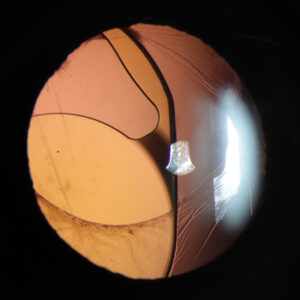
The system’s AI-guided element evaluates each individual cataract and adjusts the laser energy and pattern accordingly. In addition to cyclotorsion compensation, Dr. Shamie said the system provides accurate axis marks to align toric IOLs. This is helpful because even the patient’s referring eye doctor can check to make sure the IOL is aligned postop, visually seeing the axis nubs, if the patient is having visual disturbances postop. “All you have to say is, ‘Dilate the pupil and are the marks aligned perfectly with the nubs,’” Dr. Shamie said. She also referenced a study that showed 100% of patients who received ALLY cataract surgery with a toric IOL were within ±0.5 D of target.
Ultimately, Dr. Shamie said, “we’re not aiming with robotics to replace our favorite, trusted surgeon with a robot. What we’re aiming for is to give that surgeon a few … advantages.”

Source: ASCRS
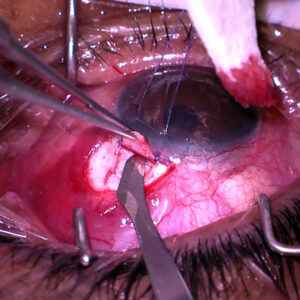
Also in the symposium, Uday Devgan, MD, described his involvement conducting the world’s first robotic-assisted cataract surgery on a human patient with the Polaris platform (Horizon Surgical Systems). He presented video of one of the first 10 robotic, in-human cataract surgeries. The video showed the robot holding the phaco probe, which Dr. Devgan was driving while looking at a screen with 3D glasses. He described the procedure as “very precise.”
“Now it’s not just about doing telesurgery. It is about making you a better version of yourself,” he said of robotic cataract surgery, adding the first 10 cases went “beautifully” with no adverse events.
One of the advantages of the robot, Dr. Devgan said, is that it has faster reflexes than a human. It’s also more precise. He later described some of the safety advantages, such as settings that would prevent the surgeon operator from coming within 5 microns of the posterior capsule. There are also protocols for measurements for incisions in exactly the right place. The robot won’t decline in skill with time/age as a human surgeon could in late career, Dr. Devgan said.
The joystick of the robot is similar to that of a phaco probe, making it natural for the surgeon operator/driver. He also showcased footage of the robot taking charge of specific parts of the surgery that were supervised visually but not driven by the human surgeon.
“This is going to change the future of how this is being done,” Dr. Devgan said, adding that he thinks it will be in surgeons’ hands before his career is up. “It can make you a better version of yourself, and it can help the rest of us operate as well as the best of us.”

Source: ASCRS
Vance Thompson, MD, asked the audience to imagine a future where every procedure was consistent, where there was less surgeon fatigue and other surgeon-limiting factors, where more patients could be helped with the fewer ophthalmologists that are projected to be available in the future.
“Surgical robotics have been around for quite some time that I’m kind of amazed that it’s taken this long to get to ophthalmology. If you think about it, we work on what most people say is the most precious sense, but there is low variability and geometry of the anatomy that we’re working on compared to other organs, and we have a fairly consistent routine. It’s high volume, and so it’s ripe for robotics and the small space that we work in,” he said.
Dr. Thompson presented on what can be expected of robotic surgery in ophthalmology, including reduced training time, lower dexterity thresholds, ease of enabling new procedures, and improved ergonomics, surgical techniques, and outcomes.
Dr. Thomspon said he has worked with the Jasper Platform (ForSight Robotics) on porcine eyes and “was amazed at how well it worked.” He also showed a video of the company’s first-in-human procedure, which was announced in April 2026. “When you wonder how long it’s going to be for robotics to be here, it’s here,” Dr. Thompson said.
In addition to these formal presentations, there was a robust panel discussion on the topic of robotic ophthalmic surgery within the symposium. Attendees of the ASCRS Annual Meeting can log in to view captured content from the symposium here.
About the physicians
Uday Devgan, MD
Devgan Eye Surgery
Los Angeles, California
John Hovanesian, MD
Harvard Eye Associates
Laguna Hills, California
Neda Shamie, MD
Maloney-Shamie Vision Institute
Los Angeles, California
Vance Thompson, MD
Vance Thompson Vision
Sioux Falls, South Dakota
Relevant disclosures
Devgan: Horizon Surgical Systems
Hovanesian: Alcon, Bausch + Lomb, Horizon Surgical Systems, and Johnson & Johnson
Shamie: LENSAR
Thompson: ForSight Robotics, LENSAR
Contact
Devgan: devgan@gmail.com
Hovanesian: johnhova@gmail.com
Shamie: ns@maloneyshamie.com
Thompson: vance.thompson@vancethompsonvision.com