Cataract
December 2020
by Ellen Stodola
Editorial Co-Director
In some cases, it may be necessary to refixate or remove an IOL after cataract surgery. Several surgeons discussed how they determine when this course of action is needed and techniques they use.

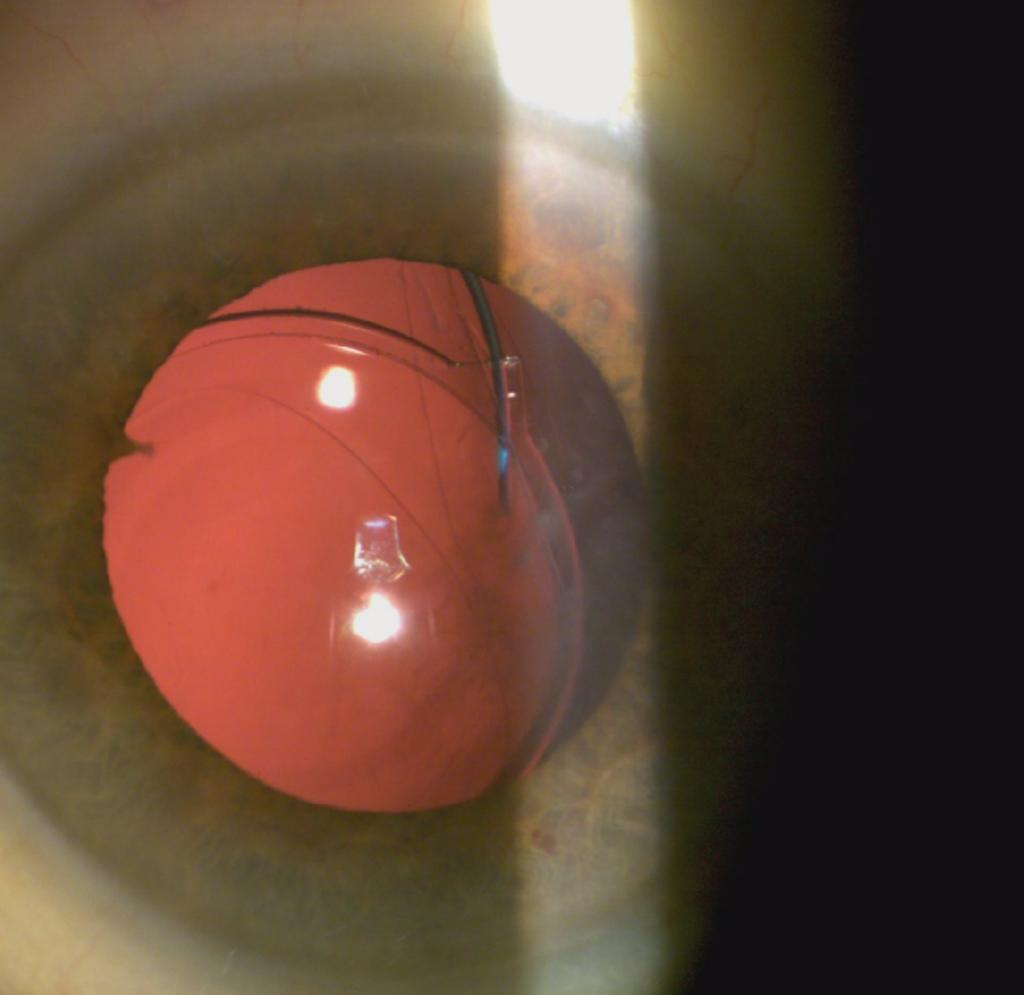
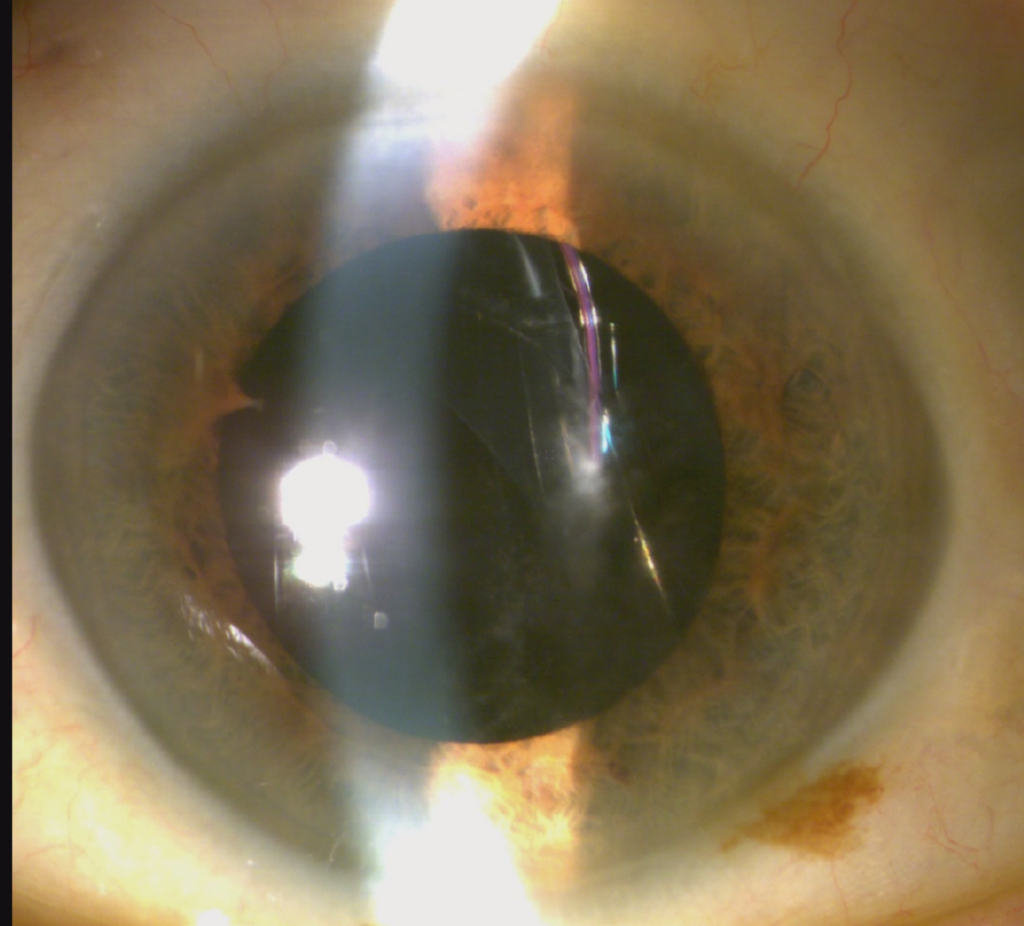
Source: Karolinne Maia Rocha, MD, PhD
When you have a patient with a dislocated lens-bag complex, there are a variety of factors to consider, said Steve Safran, MD. First, he noted that you could be dealing with dislocation of the whole lens-bag complex where the zonules are shot; he usually uses a lasso in these cases. On the other hand, the capsular bag could be intact but within the lens is dislocated. “Your decision will depend on whether or not you want to keep that lens,” Dr. Safran said.
Choosing an appropriate option depends on the anatomy, your strategy, and if the IOL inside the eye is the one you want to keep. “Most of the time, they are lenses I want to get rid of,” he said.
Dr. Safran said in rare cases, comorbidities may influence the decision. If there’s a filtering bleb, that might limit your angle of approach. If the patient is a high myope with a large eye, that will influence the decision. If the eye is bigger, it might be more difficult to do certain techniques.
In terms of determining when a lens should be repositioned vs. exchanged, Soon Phaik Chee, MD, said this will often depend on the particular IOL. The design of the haptics, IOL power, and condition of the IOL all play a role, she said. The technique for fixation will also influence the decision—for example, if the IOL can be sutured to the iris or if it’s going to be intrascleral fixation.
Dr. Chee said she will do a supine exam, if a couch is available. “However, if a UBM has been done, I do not need to lie the patient down because the scan gives an image of the IOL with the patient in the supine position,” she said.
It’s also important to consider iridodonesis. Eyes that have undergone surgeries, such as trans pars plana vitrectomy, or patients with floppy irises are more difficult to operate on, Dr. Chee said, explaining that it is difficult to suture an IOL to a floppy iris. “These eyes have more pseudophacodonesis, postoperative inflammation, and pigment dispersion that lasts for 3–4 months regardless of whether the IOL is iris sutured or enclavated,” she said. “For this reason, I prefer intrascleral haptic fixation as the IOL is rock stable during eye movements.” Dr. Chee said if an adequate peripheral iridectomy is created, and the IOL is not tilted or decentered, there is little risk of optic capture when the pupil is dilated.
Additionally, Dr. Chee said she will stop the anticoagulant to reduce the risk of vitreous hemorrhage and raised IOP when possible. Passing the needle through the iris or sclera can evoke an uncontrolled bleed and raised IOP in these compromised eyes.
Dr. Chee said she will proceed without a retina specialist if she can reach the IOL safely with micro-forceps with adequate exposure for things like iris hooks and scleral indentation. She will stain the vitreous with diluted triamcinolone acetonide to ensure she does not tug on the vitreous and clear the vitreous around the IOL before moving it to the anterior segment. “Have a vitreoretinal colleague in to assist for the less experienced and combine surgery when the IOL is in the posterior vitreous cavity or on the macula,” she said.
IOL removal considerations
Karolinne Maia Rocha, MD, PhD, said there are several reasons an IOL may need to be exchanged. First, she noted significant residual refractive error. This might be a patient who cannot be corrected with refractive surgery. These are the patients who it’s clear on postop day 1 have the wrong power IOL. “That’s when we really need to exchange that lens, when it’s the wrong lens or power or [has a] huge refractive surprise,” she said.
Another reason for exchange, Dr. Rocha said, is in a patient who has a trifocal or EDOF lens and, despite all correction of residual refractive error and/or dry eye treatment, is having significant dysphotopsia.
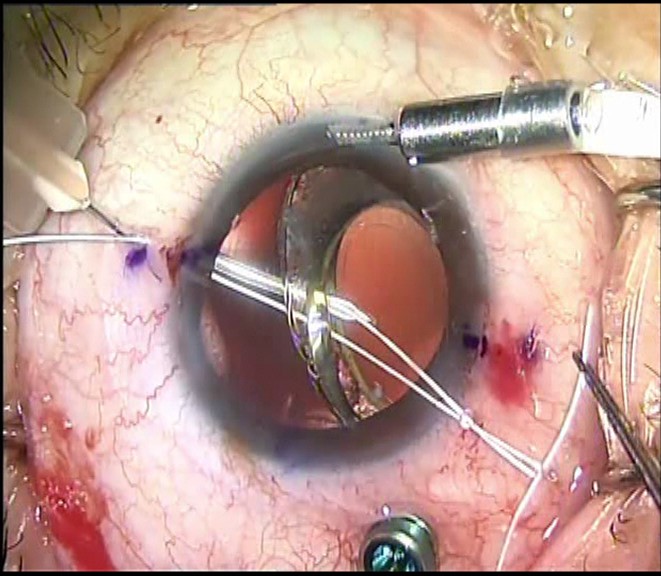
Source: Steve Safran, MD
Lastly, she noted that a lens may need to be removed if it has been dislocated with damage to the IOL, such as in a traumatic accident or pseudoexfoliation syndrome.
When performing an IOL exchange in cases where the capsular bag is intact, Dr. Rocha will use dispersive viscoelastic to try to open the capsular bag, especially around the haptics. Then she carefully prolapses the lens into the anterior chamber. She noted that this is generally easy with single-piece IOLs; this may be harder with a Crystalens (Bausch + Lomb) because of the design of the haptics.
Dr. Rocha places the new lens in the bag and cuts the original IOL in the anterior chamber; placing the new lens makes it safer to cut the exiting lens.
If the capsular bag is not intact, she checks whether the anterior capsule is intact. She said you should try to place the lens in the sulcus. A single-piece IOL should never be in the sulcus because these patients may develop pigment dispersion and UGH syndrome. A three-piece lens can be placed in the sulcus, Dr. Rocha said, noting that she likes the optic capture technique.
Dr. Safran said that many times when he is taking out an old lens, it may be scratched or the wrong power or in some cases, he doesn’t know the power. Some lens types don’t do well over time, he said, noting that he will always remove a hydrophilic acrylic lens with a problem because those tend to calcify if you do a secondary procedure.
“If the lens is dislocated with no capsule support, I’m going to cut it and take it out [and do a] pars plana vitrectomy and a Yamane technique,” he said. It works well to “clear everything out,” he said, because then you know you have the right power with a fresh lens. When you lasso an old lens-bag complex, it can be full of “junk,” Dr. Safran said, like Soemmering’s ring material, fibrosis, etc.
Additionally, Dr. Safran said that if you have a dead bag, it’s important to take this out because the bag is so fragile, and once you start passing sutures, it will likely fall apart.
Source: Soon Phaik Chee, MD
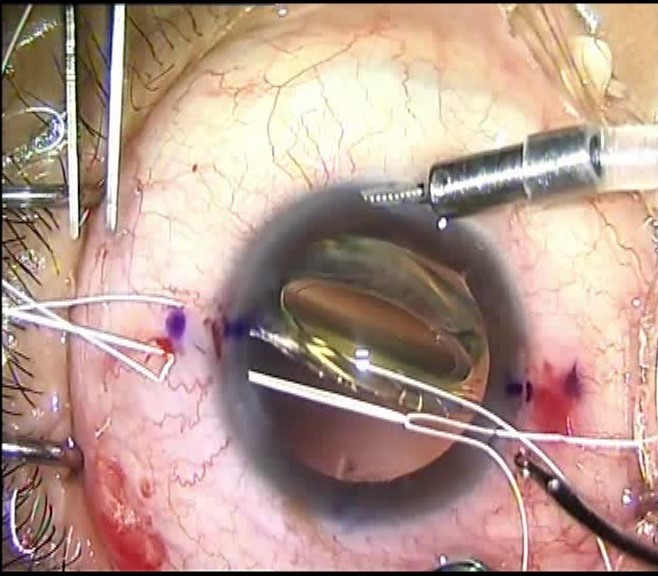
Source: Soon Phaik Chee, MD
When choosing to remove the IOL, Dr. Chee said she will use only dispersive OVD to maintain space and protect the endothelium, which is often weak in these complex eyes. “Furthermore, some OVD can safely be left in the eye without incurring a pressure spike,” she said.
When removing an IOL, Dr. Chee said she prefers to cut it rather than refold it inside the eye. She specifically discussed removal of silicone IOLs, which can be more slippery. “I grab the haptic or capsule if they are dislocated posteriorly to levitate them, rather than attempting to grasp the optic,” she said. “I prefer to explant them, as they do not stay still when attempting to iris fixate.” She’ll use serrated IOL forceps to grasp the IOL when cutting. “If you fail to hold the IOL firmly with your lens forceps, try the conjunctival forceps, which are serrated and will hold them firmly for explantation,” Dr. Chee said.
It’s important to know the IOL you’re explanting, where the positioning hole is or whether there is a knob at the end of the haptic, and what the IOL material is, Dr. Chee said.
If you need to open the capsule and free the haptics, Dr. Chee recommended inserting the OVD cannula between the anterior capsule and the IOL anterior surface. Begin injecting the OVD, but if this is not possible, she said to use a micro-grasper to lift up the anterior capsule to allow the OVD cannula to slip between the anterior capsule and IOL and inject the OVD. She said to avoid using graspers that have a sharp end, as the capsule may rip.
If the haptics are adherent and do not come free with OVD and dissection, Dr. Chee said to lift the optic out of the bag and cut out and remove the central third. You could also cut the optic in half, which allows you more room to attempt to free the IOL without stressing the zonules.
Dr. Chee said she prefers to reposition or exchange a lens that is fully in the bag earlier rather than later (and before fibrosis sets in), but she would hardly consider any IOL too late to reposition or exchange.
IOL refixation
Dr. Rocha noted that if the lens still looks good and the patient has good vision, this is a scenario when you can plan to use the same lens and refixate it. If you’re keeping the same lens, she said it’s important to determine if the patient was able to see well before with this lens and to rule out any IOL damage and determine if the patient needs a vitrectomy.
There are some single-piece IOLs that you can refixate, she said, adding that she likes to use a belt loop technique, which she noted is described in depth by Cathleen McCabe, MD. Dr. Rocha will use 6-0 Prolene with this technique and scleral fixation. She then loops the IOL haptics to the scleral wall.
If the patient has a three-piece IOL in the eye, one technique that is popular is the Yamane technique, Dr. Rocha said. She uses a toric marker at 6 and 12 o’clock and a secondary mark 2.0 mm from the limbus. Two angled scleral tunnels are made parallel to the limbus at the marked locations using two needles; she uses either a 30-gauge TSK ultra-thin wall needle for the CT LUCIA lens (Carl Zeiss Meditec) or a 27-gauge needle for the AR40E SENSAR IOL (Johnson & Johnson Vision). She then feeds the needles using micro-forceps and pulls the haptics.1
Using a glued IOL was described many years ago by Amar Agarwal, MD, Dr. Rocha said, mentioning this as another option.
Choosing a technique depends on the IOL type. If the patient has a PMMA lens, this has a little hole that you can move and perform a scleral fixation with either 6.0 Prolene (the belt loop technique) or Gore-Tex CV-8. Another option is iris fixation, but she said she’s “not a big fan because we usually see a lot of pigment dispersion and sometimes CME.” With a three-piece IOL, you can do iris suture/iris fixation, if you’re using the same lens, she said.
If the whole lens complex is dislocated but the lens is in the bag and looks like it’s a good lens, Dr. Safran said he will lasso the whole lens bag complex. He uses Gore-Tex sutures with a lasso in these cases. In most of these patients, Dr. Safran said he will also do a vitrectomy. “If you don’t do the vitrectomy, you can get burned,” he said. It’s easy to inadvertently engage vitreous when passing a suture through the capsular bag and bring vitreous forward into the anterior segment, he explained, emphasizing the importance of avoiding vitreous traction to the lens or sutures.
Dr. Chee discussed using a lasso technique and said she creates belt loops around the haptics of the IOL either with or without a CTR only if they are still within the capsular bag. “I use either Prolene 6-0 suture with the McCabe technique or Gore-Tex CV-8 suture (which is off label for ophthalmic use) using the suture snare technique, employing Hoffman pockets,” she said. For both the McCabe and suture snare techniques, Dr. Chee said she uses a 27-gauge needle to pierce the capsular bag to lasso the haptic. “I use a capsulorhexis micro-forceps to grasp the capsular bag to position it when piercing with the needle,” she said. These are simple techniques to master, she added, and the position of the sclerotomies are determined by the remaining zonules (if any). When fixing both ends, Dr. Chee said they should be positioned diametrically opposite from one another.
The Yamane technique or a glued IOL technique are other options for refixating the IOL. Dr. Chee said she has learned never to reuse the existing IOL for intrascleral haptic fixation. Instead, she exchanges them for either a CT LUCIA 202 or 602 with PVDF haptics or the AR40E SENSAR lens with PMMA haptics. She added that both Hoya and Santen make IOLs with longer PVDF haptics specifically for intrascleral haptic fixation, but they are only available in Japan.
If some capsule support remains, the surgeon may choose to iris fixate an existing three-piece lens. Dr. Chee said she does not opt for iris fixation unless there is some capsular support. She added that one potential downside is that iris fixated IOLs may dislocate years later in patients who chronically rub their eyes. Iris fixation may also incur a cat’s eye pupil, she said.
Postoperative considerations
Some patients may require follow-up with a retina specialist. “All these complex surgeries that incur vitreous removal can pose a risk to the retina,” Dr. Chee said. “I generally will give the patients the necessary advice and screen their retinas starting as early as 10 days postoperatively and at almost every consult. I only refer if I am suspicious of a retinal problem.” She added that when dealing with a highly myopic eye that is at an increased risk of IOL subluxation, she prefers that the retina surgeon screen the eyes for retinal breaks prior to surgery. “I also perform OCT of the macula if the vision is not as good as expected to detect and treat CME early.”
Dr. Chee said it’s also important to look out for raised IOP, persistent inflammation, and endothelial cell loss, in addition to retinal issues.
In terms of medications to use, Dr. Chee said that with intrascleral haptic fixation, the inflammation resolves within a month, and using topical steroids, antibiotics, and a topical NSAID for 1 month is adequate. With iris fixation, these eyes require the same medications but sometimes for 3–4 months after surgery.
Dr. Rocha noted that she uses the same drops that she uses for regular cataract patients. But she watches for CME postop especially in iris fixated lenses, she said, adding that it’s also important to monitor for IOP spikes.
ARTICLE SIDEBAR
Cutting IOLs
One important thing to know when planning to cut IOLs is that it is hard to cut a PMMA lens, Dr. Rocha said. However, for hydrophilic or hydrophobic lenses, you can cut them in the anterior chamber and remove them through the small incision.
To remove PMMA lenses, Dr. Safran said he makes a 6-mm scleral tunnel on the steep axis with a self-sealing incision. You can put pars plana trocars in and an infusion line to keep the eye firm, he said. If it’s PMMA, it should come out in one piece, Dr. Safran said. Though he said that he sometimes will cut the haptic and go after those separately.
Dr. Safran said that “all of the foldable lenses,” including hydrophilic acrylic, hydrophobic acrylic, or silicone, should cut readily.
Dr. Chee also shared some tips for cutting IOLs. If possible, she said to mobilize the IOL into the anterior chamber to cut in order to avoid capsular injury. She also said to ensure that the entire capsular bag is bowed posteriorly with OVD to prevent both anterior and posterior capsule injury, as OVD may be lost during the cutting process. “This is especially important when cutting the optic if the entire IOL cannot be mobilized into the anterior chamber,” she said. “Make sure that the tip of the scissors does not cut the capsulorhexis rim.” Another technique for reducing the risk of posterior capsule injury is to insert the new IOL into the capsular bag, under the old IOL. Dr. Chee said the new IOL acts as a scaffold to protect the posterior capsule while the old IOL is being cut in the anterior chamber.
She said to use intraocular scissors that are intended for the purpose and ensure they are sharp. Grasp the IOL firmly with intraocular forceps when cutting. Or you could provide a counterforce opposing the cutting force to prevent the IOL from slipping. Dr. Chee said to ensure that no sliver of the IOL is left in the eye during the cutting process.
Dr. Chee said that the IOL can be cut into two or three pieces, depending on the incision size desired. “A useful technique that avoids the need to rotate one half of the IOL during explantation to avoid the haptic snagging the intraocular structures is to use the ‘Pacman’ method,” she said. “This involves cutting the IOL three-fourths across and rotating the cut section followed by the rest of the IOL out through the incision.”
The way an IOL behaves when cut also depends on the IOL material. Dr. Chee said the AcrySof IOLs (Alcon) tend to be thinner, softer, and easier to cut than the thicker, more rigid TECNIS IOL (Johnson & Johnson Vision). She added that hydrophilic IOLs are softer, thinner, and easier to cut across and can be removed through a smaller incision than hydrophobic IOLs. However, silicone IOLs are slippery and thick and are the most difficult to explant.
About the physicians
Soon Phaik Chee, MD
Singapore National Eye Centre
Singapore
Karolinne Maia Rocha, MD, PhD
Director of Cornea and
Refractive Surgery
Medical University
of South Carolina
Charleston, South Carolina
Steve Safran, MD
Lawrenceville, New Jersey
Reference
- Rocha KM, et al. Combined flanged intrascleral intraocular lens fixation with corneal transplant. Am J Ophthalmol Case Rep. 2018;13:1–5.
Relevant disclosures
Chee: Carl Zeiss Meditec, Johnson & Johnson Vision, Hoya Surgical Optics
Rocha: None
Safran: Johnson & Johnson Vision, Cynosure
Contact
Chee: chee.soon.phaik@singhealth.com.sg
Rocha: karolinnemaia@gmail.com
Safran: safran12@comcast.net



