Glaucoma
Spring 2026
by Ellen Stodola
Editorial Co-Director
The suprachoroidal space is an unmastered surgical pathway to reduce IOP, said Emily Schehlein, MD. “Surgical intervention in the suprachoroidal space is not new; Leopold Heine introduced the idea that this procedure could be used as a treatment for glaucoma in 1905,” she added.1
Dr. Schehlein and Lori Provencher, MD, discussed benefits to expanding access to the suprachoroidal space, which patients might benefit the most, and other important considerations.
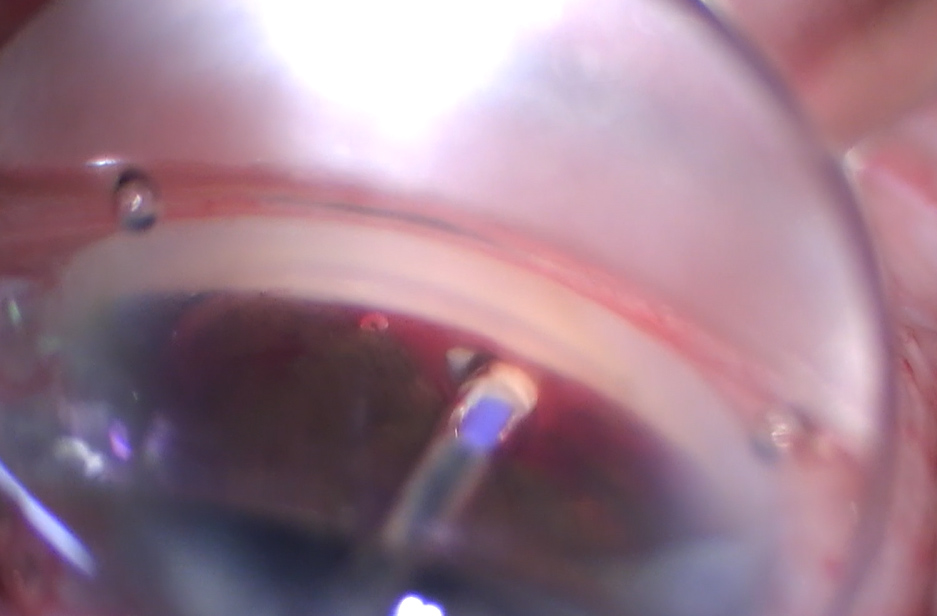
Source: Emily Schehlein, MD
Dr. Schehlein said that minimally invasive glaucoma surgery has renewed interest in surgeries that are successful in lowering IOP, sparing the conjunctiva, and avoiding complications attributed to blebs. “While most MIGS act on the conventional outflow pathway (trabecular meshwork, Schlemm’s canal, distal collector channels, veins), the uveoscleral pathway is gaining attention for surgical augmented outflow,” she said. “This pathway has been traditionally thought to drain 10–15% of aqueous humor but has been shown to do much more, potentially up to 50–60% depending on age and other factors.”2
She added that the goal is suprachoroidal surgeries that are safe, efficacious, and predictable.3 “We still need randomized clinical trials and basic science research to elucidate much about suprachoroidal fibrosis and cleft closure,” she said.
Dr. Provencher said there are a variety of options to optimize the trabecular outflow system, through stenting, viscodilation, and/or excision procedures. “Since the recall of the CyPass [Alcon], we have not had a surgical option to access suprachoroidal outflow,” she said. “Ironically, our most prescribed first-line medical option, prostaglandin analogs [PGAs], targets this system. PGAs do a beautiful job of lowering IOP, but topical PGAs have some of the worst local side effects of our topical options.”
She also mentioned that the uveoscleral system may contribute to around 50% of outflow. “We also know that this is a pressure-independent system, with no episcleral venous pressure floor and hence, the potential to achieve lower IOPs,” she said. “It is also agnostic of prior trabecular meshwork-based procedures. It’s no surprise that glaucoma specialists have been dreaming of an option to access this space again.”
Which glaucoma patients would this be best for?
Suprachoroidal procedures fill a glaring unmet need, Dr. Provencher said, adding that these could potentially help the patient who is post-trabecular meshwork intervention but does not warrant a minimally invasive bleb surgery (MIBS), trabeculectomy, or tube, i.e., filtration surgery. “Traditionally, these post-trabecular meshwork MIGS patients would go back on medications and progress until their disease ‘warranted’ the risk of filtration,” she said. “Now, with suprachoroidal stents, we can do another safe, minimally invasive procedure that opens the ‘second drain’ of the eye, allowing us to stay ahead of progression, which aligns with the principles of interventional glaucoma.”
Dr. Schehlein offers these procedures to patients who have exhausted other MIGS procedures and are facing an incisional glaucoma procedure, like a tube or trabeculectomy, in the future. “As we gain more experience with various devices, targeting the suprachoroidal space may move earlier in our glaucoma treatment regimen,” she said.
Available procedures and devices
Currently, Dr. Provencher said there is one option, cyclodialysis cleft creation and reinforcement with the AlloFlo Uveo (Iantrek). This is an allogenic processed scleral tissue stent that scaffolds open an intentionally created cleft. “The perfect tissue match to the surrounding native sclera is designed to induce little to no inflammation and/or fibrosis of the cleft,” she said.
A side port incision and clear corneal temporal incision (Dr. Provencher uses a 2.4 mm keratome) is created. Then, she said the AC is filled with cohesive viscoelastic, adding that this is a better tamponade of bleeding. “Under a gonioscopic view, you create a 1-clock hour cleft by strumming posteriorly on the scleral spur with a cannula or cyclodialysis spatula,” Dr. Provencher said. “Think of the cannula (or spatula) following the curve of the sclera. You will see the white scleral back wall if you are in the right space. Fill this space with additional viscoelastic. You then enter the AC with the AlloFlo Uveo, insert it into the cleft, and retract the sleeve, which deploys the stent.” She added that you want about 0.5 mm of stent in the AC, and the position can be adjusted easily by tapping it in farther with the inserter or pulling it out with a cystotome. “You can then expand the cleft and add another stent at the other margin of the cleft,” she said. “Currently, I use two stents with 1–1.5 stent widths in between. Remember, these stents are designed primarily as scaffolds, though they do transmit fluid. You may encounter bleeding, but it rinses out with I/A.” She added that postoperative hyphema is rarely significant.
For cleft creation (if not being done with the stent handpiece or inserter), there are several instruments that can be used, Dr. Schehlein said. “Some surgeons may choose to create a cleft simply with the viscoelastic cannula, however, a Koch spatula or cyclodialysis spatula can also be suited for adequate cleft creation,” she said.
Dr. Schehlein also cautioned that cleft creation can be difficult, and it may feel counterintuitive. However, she said that the structure of the cleft is important in procedure success. “Visually, surgeons should see the underside of the scleral wall (white),” she said. “After cleft creation, surgeons can dilate the cleft with viscoelastic to enlarge the cleft and tamponade heme.”
Dr. Schehlein said that surgeons who had the opportunity to work with the CyPass will be comfortable in this space, but younger surgeons who missed the on-market window may not have experience in the suprachoroidal space. “While cleft creation and stent insertion may have a learning curve, any surgeon who is comfortable with intraoperative gonioscopy and working in the angle can dive into this space,” she said.
Dr. Schehlein said some surgeons may create a cyclodialysis cleft prior to suprachoroidal stent implantation, while others may choose to use the device to create the cleft and inject the stent at the same time. She also noted a review that she was an author on, which mentions the iStent Supra (Glaukos) and the MINIject drainage system (iSTAR Medical), as well as what is now the AlloFlo Uveo. Currently, only the AlloFlo Uveo is available in the U.S.4
Other considerations in the suprachoroidal space
As with many MIGS, postoperative IOPs spikes can occur, Dr. Provencher said, particularly within the first 30 days. She added that keeping patients on their glaucoma drops can help. “The spikes are usually short lived and controllable,” she said. “If a patient’s visual field would not tolerate a brief IOP spike, I would not recommend trabecular meshwork-based interventions or suprachoroidal stenting. These patients are better served with filtering procedures.”
Dr. Provencher also noted that she likes to prescribe 1 week of antibiotic drops, along with a steroid taper over a few weeks. “I have found it’s also very helpful to keep patients on a prostaglandin analog to optimize uveoscleral outflow,” she said.
“The [CyPass] reduced endothelial cell count (ECD) and was removed from the market,” Dr. Schehlein said. “We now know this occurred when the device was not in its optimal position, however, there is limited published long-term data on ECD and any MIGS device, including those in the suprachoroidal space. ECD loss can be accelerated by glaucoma surgery, so the positioning of any suprachoroidal device will need to be appropriate.”5,6,7
She said it’s also important to be cognizant of the patient’s stage of glaucoma and current medications. Acute cleft closure with severe pain seems to be less common with these procedures, but if a suprachoroidal stent fails and the cleft closes, the patient’s pressure can increase significantly. “It is prudent to keep patients on their medications if preoperative IOP is high, especially a prostaglandin analog (which will increase uveoscleral outflow) after surgery,” Dr. Schehlein said. Some surgeons may also consider placing the patient on pilocarpine postoperatively with the goal of maintaining the cleft.
Dr. Schehlein added that patients can sometimes have more sensation during procedures in the supraciliary space, and it may be necessary to give additional systemic anesthesia and/or consider a sub-Tenon’s or retrobulbar block.
About the physicians
Lori Provencher, MD
Cataract Surgeon and
Glaucoma Specialist
Vance Thompson Vision
Omaha, Nebraska
Emily Schehlein, MD
Glaucoma Specialist
Brighton Vision Center
Brighton, Michigan
References
- Böke H. [History of cyclodialysis. In memory of Leopold Heine 1870–1940]. Klin Monbl Augenheilkd. 1990;197:340–348.
- Toris CB, et al. Aqueous humor dynamics in the aging human eye. Am J Ophthalmol. 1999;127:407–412.
- De Francesco T, Ahmed IIK. Surgical augmentation of the suprachoroidal space: a novel material and implant. Clin Ophthalmol. 2023;17:2483–2492.
- Schehlein E, et al. Emerging minimally invasive glaucoma devices and sustained delivery platforms – what is in the pipeline? Curr Surg Rep. 2024;12:326–332.
- Ahmed IIK, et al. Corneal endothelial safety profile in minimally invasive glaucoma surgery. J Cataract Refract Surg. 2024;50:369–377.
- Lass JH, et al. Corneal endothelial cell loss and morphometric changes 5 years after phacoemulsification with or without CyPass Micro-Stent. Am J Ophthalmol. 2019;208: 211–218.
- Fili S, et al. [Explantation of the CyPass implant in a case series of patients with corneal decompensation]. Ophthalmologe. 2021:118;42–49.
Relevant disclosures
Provencher: AbbVie, Alcon, Bausch + Lomb, BVI, Elios, Glaukos, Iantrek, Microsurgical Technologies, New World Medical, Radius, RxSight, Thea, Vialase, Zeiss
Schehlein: Alcon, AbbVie, Glaukos, Iantrek, Nova Eye Medical
Contact
Provencher: lorrainemprovencher@gmail.com
Schehlein: emschehlein@gmail.com


