Dry Eye and Ocular Surface Disease Bonus Issue
October 2025
by Liz Hillman
Editorial Co-Director
The ocular surface impacts many ophthalmic subspecialties beyond cornea. Whether it’s within refractive surgery or cataract surgery, glaucoma therapy or retina procedures, the ocular surface can affect outcomes and quality of life for patients being treated by these subspecialists. On the flip side, the procedures within these subspecialties can cause or exacerbate ocular surface issues themselves.
Several anterior segment ophthalmologists spoke with EyeWorld about the ocular surface and how it relates to their subspecialty.
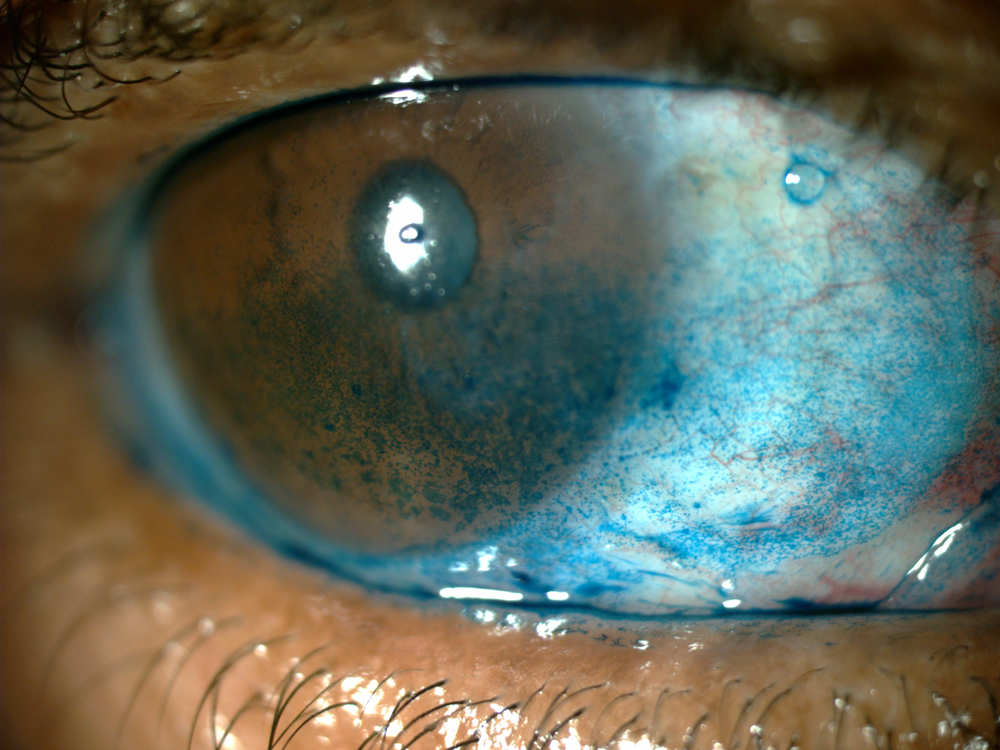
Source: Eric Donnenfeld, MD
The cornea perspective
Awareness of the impact of ocular surface disease across the subspecialties has improved drastically in the last few decades, especially as more diagnostic capabilities and diverse treatment modalities became available, said Kenneth Beckman, MD.
As the impact of the ocular surface on refractive outcomes of cataract surgery became more well known, especially with advanced- technology lenses, knowledge and subsequent treatments have trickled down the ranks from cornea specialists to cataract and refractive specialists. Dr. Beckman said that oculoplastics, glaucoma, and retina physicians are becoming more aware of how their medications and procedures affect the ocular surface of patients.
“From a plastic standpoint, they’re doing a lot of lid lifts in one fashion or another. You’re getting greater exposure and dry eyes,” Dr. Beckman said. “With glaucoma, they’re on multiple medications that can be toxic with prolonged use. They’re having surgical procedures that are altering the surface. Those things all can lead to dry eye. With the retina specialist, it’s the same thing. These are patients who are getting multiple interventions—injections, vitrectomies—and you’re altering the surface. All of those fields, while they’re not necessarily dealing with visual acuity per se, are impacting visual acuity by impacting dry eye.
“They may not even be managing the dry eye, but a lot of times they’re seeing the patients far more often than the comprehensive ophthalmologist who refers them out, so they’re getting the complaints,” he continued. “They have to be prepared to handle these patients because they’re not going to want to keep sending them back to me.”
Here’s Dr. Beckman’s message, as a cornea specialist, to ophthalmologists in the other specialties:
- Glaucoma: Consider SLT or another glaucoma intervention instead of another harsh drop. Consider preservative-free drops.
- Retina: If you want the patient on a non-steroidal, consider bromfenac, which can be used less frequently and is less toxic on the surface, rather than ketorolac. If an antibiotic is needed, consider a lower toxicity drop such as gatifloxacin rather than combination drops such as neomycin/polymyxin. Newer treatments that could reduce injections, and thus the betadine prep, could be helpful as well.
- Oculoplastic: In cases of blepharoplasty or ptosis repair, oculoplastic surgeons should mention to patients the dryness that may occur afterward due to increased surface exposure or an incomplete blink. Be conservative with your surgery, especially in patients who have pre-existing dry eye. Patients with thyroid eye disease already might be suffering from exposure, and Tepezza (teprotumumab, Amgen) could be helpful.
Dr. Beckman’s general take-home points include:
- Be aware of problems that you’re not treating and how your treatment could impact them. “If I sent a Sjögren’s disease patient to a glaucoma specialist, I don’t want you to do something to make their surface worse if it can be avoided.”
- Be aware in someone who doesn’t have any underlying problems how your treatment could kickstart ocular surface issues.
The cataract perspective
Offering the cataract perspective, Su Jeoung Kim, MD, Lucy Li, MD, and Aakriti (Aaki) Garg Shukla, MD, MSc, together provided thoughts on the importance of the ocular surface.
They said to pay close attention to the patient’s ocular symptoms and complaints, such as that of intermittent blurry vision, burning, watering, or itching. The physicians said they examine the patient’s lids, conjunctiva, and ocular surface, looking for tear instability and signs of inflammation. In addition to dry eye disease, they’re looking for epithelial basement membrane dystrophy, Salzmann’s nodular dystrophy, pterygia, and conjunctivochalasis.
Drs. Kim, Li, and Shukla said they ask about a history of autoimmune conditions and prior contact lens use or laser refractive surgery like LASIK or PRK. “Treating these corneal pathologies prior to the cataract surgery is very important because they can lead to postop refractive differences of 1 D or more,” they noted.
If ocular surface issues are identified, the physicians said they explain to the patient that they have two different conditions—the cataract and an ocular surface abnormality, both of which require treatment. “Some patients are surprised initially to find that these treatments can delay their cataract surgeries. In these cases, patient education is key to help them understand the goals and expectations of these ocular surface treatments from the start. Once the patients understand how and why these issues are treated, they will be much more willing to undergo the preoperative treatments for a few weeks to improve their outcomes and quality of life,” they said.
If ocular surface issues go unresolved, Drs. Kim, Li, and Shukla said it can significantly influence refractive outcomes after cataract surgery. “There are likely multiple reasons that these ocular surface issues are not fully addressed preoperatively. One is that these diseases present with varying signs and symptoms. The other is that there are no standardized diagnostic criteria for these conditions. But it is important for us to realize that not treating these conditions can lead to several unanticipated issues down the road. This includes patient dissatisfaction and worsening of certain conditions such as dry eye disease. It may even require additional postop visits to address these issues properly. Minimizing ocular surface issues will be beneficial to patients and improve their postoperative satisfaction and quality of life.”
Beeran Meghpara, MD, said that he thinks that while the impact of the ocular surface on cataract surgery outcomes is well known, it remains under treated. Dr. Meghpara ideally begins his examination of a cataract patient before they have any drops in their eye, looking at them in a systematic way similar to the flow of the ASCRS Preoperative OSD Algorithm. It takes about 30 seconds to go through the look, lift, pull, push portion of the examination prior to administering fluorescein staining. “I think this is one of the misconceptions. We’ve got this big algorithm … but it doesn’t take a long time to go through it,” he said.
If you find dryness—and the reality is everyone has at least a little bit of dryness, Dr. Meghpara said—treatment is individualized based on the patient’s level of dryness. We don’t want the dryness getting worse after cataract surgery, and we want the patient to have the best IOL calculations, he said.
He added that the cataract severity can influence how long he’ll treat the patient’s ocular surface. “If they have a terrible cataract and can’t see, it’s restricting their lives, we want to get them rehabilitated more quickly,” he said, noting that he may not strive for perfection in these cases but does want to see some kind of improvement. If a patient wants a multifocal or toric lens, he’s more persistent at achieving a pristine ocular surface preop. The clinical impact of dryness on cataract outcomes depends on the type of lens the patient is getting, Dr. Meghpara said.
Dryness that’s not addressed preoperatively can also affect the patient’s quality of life postop. “If you have staining in the middle of the cornea or a rapid tear breakup time, patients are not going to have the vision that they were hoping for. It’s going to affect contrast. It’s going to create glare, overall blurriness, and fluctuating vision that’s worse at the end of the day. Overall, the quality of vision is not going to be good, and patients will look at your cataract surgery as a failure even though the surgery itself was perfect,” Dr. Meghpara said.
He emphasized the importance of preop education on the presence of dry eye before their cataract surgery, how if untreated preop it could affect their outcomes, and how if untreated postop, it could affect their quality of vision and quality of life.
Putting on his cornea specialist hat, Dr. Meghpara said no matter what subspecialty you are, the ocular surface may not be front of mind, but it should be on everyone’s mind. “It’s important to be aware that what I’m doing is probably going to impact the ocular surface and not in a negligible way,” he said. This is especially true for vision-preserving retinal injections or glaucoma drops, both of which can have a significant impact on the ocular surface.
“Everyone has the same ultimate goal, which is to improve the overall health of the patient’s eye. But it’s a constant battle that, as these patients get older, is going to get more difficult to deal with,” he said.
The glaucoma perspective
Reena Garg, MD, said the mindset regarding the ocular surface for glaucoma patients has changed over the years—even for herself. She recalled a patient she saw while in fellowship who was begging her fellowship director to put him on a different drop due to his ocular surface issues.
“We were in the waiting room in front of all the patients, and he stopped her after his visit and said, ‘Look at me.’ She said, ‘I’m sorry, we talked about this. Your pressure is good, and they don’t make a preservative-free formulation.’ I remember at the time thinking, ‘His pressure is good; he should be happy he’s not having a trabeculectomy or a shunt. He’s one of the lucky ones, well managed on drops.’”
That used to be the mentality, Dr. Garg said—your pressure is good, you’re not going blind, so you have to deal with the side effects.
The renaissance, as she put it, started 4–7 years ago. Not only did the COVID era have people looking at their screens, exacerbating dry eye problems, and looking at themselves more, but more alternatives for glaucoma treatments have entered the market, both as medications and procedures.
“We’ve shifted in that we have safer minimally invasive surgeries. We have additional dry eye treatments that can combat some of the effects of the glaucoma medications that we’re using. I do think that changes the way we think of glaucoma management now,” Dr. Garg said. “Instead of committing patients to medications that we know are going to create ocular surface disease … we now have the flexibility to offer them other solutions, and we can think about the lifestyle component as actually important. … We can keep you under control and protect your optic nerve from glaucoma, but we also don’t have to compromise on the physical attributes or feelings from being on drops.”
Dr. Garg said ocular surface disease should absolutely be accounted for when choosing glaucoma treatments for patients, while still prioritizing health of the optic nerve. Dr. Garg tries to partner with colleagues who have a specialty in dry eye as well as referring optometrists to have a synergistic, co-management relationship. This is beneficial both for more frequent pressure checks and dry eye management. Sometimes these patients are referred by the co-managing doctor back to her for a possible change in glaucoma treatment due to ocular surface intolerance. She finds this relationship helps prepare patients for more interventional glaucoma procedures.
She said that while interventional glaucoma procedures can help patients reduce or eliminate drops, which can, over time, improve their ocular surface, sometimes these procedures immediately postop disrupt the ocular surface. “Often that’s a delayed gratification [for dry eye relief],” she said.
Dr. Garg said she does prescribe some anti-inflammatory drops and dry eye therapies, but she always tells her patients that they’d be better served by a specialist in this area. “I just dabble to help my patients because I don’t want them to suffer,” she said.
In the clinic, Dr. Garg’s first step is to ask patients how their eyes are feeling and how their drops are treating them. Then she follows up based on their complaints and how compliant they seem to be. “In the past it used to be a pressure threshold. It used to be a visual deterioration threshold for intervention or advancement of your treatment, but now it’s not so. Now it’s even if the patient is stable, if they’re miserable, we have options to offer them.”
Dr. Garg said the safety profile of minimally invasive procedures are such that if a patient has great pressure and a stable field, stable optic nerve but they’re miserable, they can be offered SLT, iDose TR (travoprost intracameral implant, Glaukos), and other things to help get them off the medications and keep them stable.
The refractive perspective
The ocular surface is incredibly important for success with refractive surgery, said Lance Kugler, MD. “What I tell patients is that 100% of the light that enters the eye travels through the tear film first,” he said.
He explains to patients that as one of the most important refractive elements of the eye, the tear film and ocular surface have to be in good shape, or no procedure will produce the results they’re hoping for.
Dr. Kugler evaluates the ocular surface preop, looking at the slit lamp, tear breakup time, tear film index with the HD Analyzer (Visiometrics), interferometry with the TearScience LipiView (Johnson & Johnson Vision), meibomian glands, and epithelial mapping. Dr. Kugler said he thinks epithelial mapping is the most important thing to evaluate the ocular surface. “[It] shows us what’s actually happening physiologically to the ocular surface that’s dry,” he said. “It’s pretty rare to see an eye with significant tear film abnormality that has a normal epithelial map, so it’s a very good test.”
If there is irregularity on the epithelial map, if the meibomian glands are in poor shape, if the tear film aberrometry is low, if any of these things are significant, Dr. Kugler said the ocular surface should be rehabilitated as much as possible before proceeding with surgery. In his practice, a procedural recommendation is not even made until the ocular surface is in good shape.
If the ocular surface is inconsistent, could an IOL or ICL-based refractive procedure be considered instead? Dr. Kugler said, in some cases, yes, because these have less of an impact on the ocular surface in the short term. However, repeatability in measurements for these procedures continues to be important for positive outcomes.
When it comes to ocular surface rehabilitation, Dr. Kugler said his practice has a comprehensive dry eye service that has many treatments and modalities available, including medications, drops, nutritional supplements, autologous serum tears (which he noted is “probably the most powerful tool we have for the ocular surface”), and devices, which include intense pulsed light therapy and BlephEx. “We treat blepharitis and Demodex very aggressively,” he said.
Once the patient has been through an ocular surface rehabilitation program, Dr. Kugler said he wants to see any tests that were abnormal prior stabilize as much as possible before proceeding. “If the ocular surface is irregular, you want to make it as regular as possible. If there are objective findings of Demodex, you want to make sure those have resolved,” he said. Dr. Kugler acknowledged that some things won’t resolve with treatment, such as meibomian gland atrophy, but optimize the surface as much as possible.
Dr. Kugler’s ocular surface management doesn’t stop after the procedure is complete. He said it’s important to pay close attention to these patients postoperatively and continue optimizing the surface as much as possible. He said it’s important to document and discuss surface irregularities preop so the patient can understand these are chronic problems that were not caused by surgery and that they require management before and after surgery.
“Patients understand that you’re going to have periocular irritation and ocular surface irregularity around refractive surgery. What they’re comforted by is knowing that you have a plan for it. If you see them and say, ‘Your surface is drier than average right now, but that’s OK. Here’s the plan where we’re going to prevent it from getting worse,’ they’re usually very receptive to that,” Dr. Kugler said.
He also said these patients are usually very compliant with postop ocular surface therapies. “They’re thrilled with their new refractive surgery eyes, and they want to keep them healthy,” Dr. Kugler said.
About the physician
Kenneth Beckman, MD
Director of Corneal Surgery
Comprehensive Eyecare of Central Ohio
Westerville, Ohio
Reena Garg, MD
Visionary Eye Doctors
Rockville, Maryland
Su Jeoung Kim, MD
Cornea Fellow
Columbia University Irving Medical Center
New York, New York
Lance Kugler, MD
Kugler Vision
Omaha, Nebraska
Lucy Li, MD
Glaucoma Fellow
Columbia University Irving Medical Center
New York, New York
Beeran Meghpara, MD
Director of Refractive Surgery
Co-Chief of the Cornea Service
Wills Eye Hospital
Philadelphia, Pennsylvania
Aakriti (Aaki) Garg Shukla, MD, MSc
Leonard A. Lauder Associate Professor of Ophthalmology
Glaucoma Division
Columbia University Irving Medical Center
New York, New York
Relevant disclosures
Beckman: AbbVie, Alcon, Amgen, Bausch + Lomb, Théa, Viatris
Garg: AbbVie, Glaukos
Kim: None
Kugler: None
Li: None
Meghpara: None
Shukla: AbbVie, Alcon, Théa
Contact
Beckman: kenbeckman22@aol.com
Garg: ragarg927@gmail.com
Kim: sk5624@cumc.columbia.edu
Kugler: lkugler@kuglervision.com
Li: lucysfmatch@gmail.com
Meghpara: bmeghpara@willseye.org
Shukla: ag2965@cumc.columbia.edu

