Refractive: Changing mindsets
Summer 2025
by Liz Hillman
Editorial Co-Director
Hydrophilic, hydrophobic, silicone, PMMA, collamer—there are many different types of IOL materials and, in the opinion of Yuri McKee, MD, “too little attention is paid to IOL material by surgeons.”
“Also, so much of what many surgeons know is from the marketing department of IOL manufacturing companies,” Dr. McKee said in an email to EyeWorld. “Many surgeons find their favorite IOL and defend the use of the lens and the material. I enjoy not being bound to any one company so that I can choose the best IOL and material for each patient. In cases of unhappy patients who require an IOL exchange, I almost always end up changing the IOL material.”
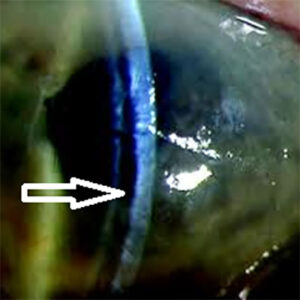
Source: Mark Gorovoy, MD
Gary Wortz, MD, expressed the importance of having tempered comments in public forums against a material. “I think we have to remember that medical decisions are made in the best interest of the patient always. It’s hard to paint a technology with a wide brush, saying you should never do X, Y, or Z or should always do this, that, or the other,” Dr. Wortz said. He also said there is no perfect lens material.
“They all have their pros and cons, and I think all the materials that we’re working with right now are great. If they weren’t great, I think they wouldn’t be FDA approved. We have the advantage of having a very strict FDA that puts materials and products through rigorous testing,” he said.
Hydrophobic acrylic
Dr. McKee called this “the current king of IOL materials,” due to its ubiquitous use among several IOL companies. Dr McKee said the higher refractive index of the material allows for a thinner IOL and smaller incision sizes.
“The simplicity, durability, small incision size, and common availability have made the single-piece hydrophobic acrylic IOL the most common IOL type in the U.S.,” he said, noting downsides have been the square-edge design of some IOLs, which were thought to decrease PCO rates but have, in some cases, increased the risk of UGH syndrome and dysphotopsia.
Dr. Wortz said hydrophobic acrylic IOLs have lower risk of PCO than hydrophilic acrylic IOLs, but he noted some issues with glistenings.
“It’s not all materials, but I think some of the hydrophobic acrylic materials may have a bit more propensity for negative dysphotopsias. The Abbe numbers are a bit on the lower end, and their index of refraction tends to be on the higher end, and that can cause negative dysphotopsias and chromatic aberrations,” he said.
Dr. McKee said he now mostly uses hydrophobic IOLs and avoids hydrophilic due to a high rate of IOL opacification in eyes with prior pars plana vitrectomy, uveitis, air injections, and other conditions. “The risk of long-term complications is simply too high for my comfort with hydrophilic IOLs,” he said. “I do not think this risk is avoidable, and I no longer consider IOLs of this material for implantation.”
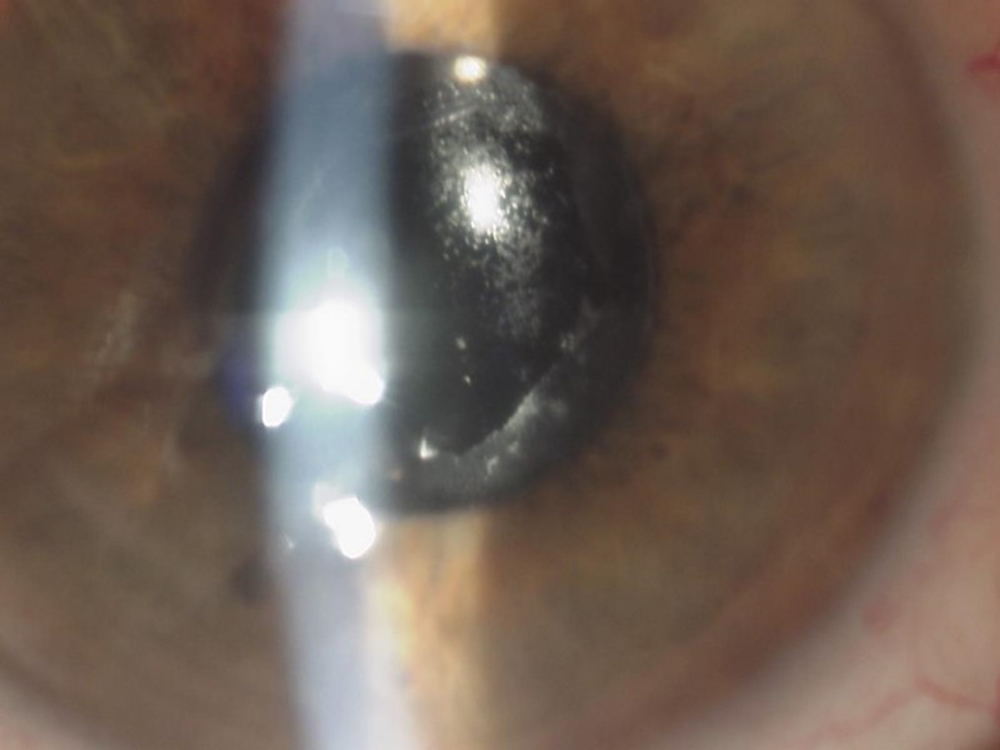
Mark Gorovoy, MD, said he is opinioned in favor of hydrophobic IOLs. As a referral-based practice, many of which are for explantations, Dr. Gorovoy said he sees calcified hydrophilic lenses “very frequently,” after secondary procedures such as tissue transplants or retinal issues. As such, he thinks hydrophilic lenses should be contraindicated, with hydrophobic lenses considered instead, for patients who might need an air bubble with DMEK or who have a history of retinal problems.
Glistenings that have been associated with hydrophobic lens materials, such as the AcrySof platform (Alcon), Dr. Gorovoy said, have been replaced with a new hydrophobic material (Clareon, Alcon), which appears to be glistening-free. Dr. Gorovoy said time will tell if this material remains glistening free. On the topic of glistenings, Dr. McKee said the enVista platform (Bausch + Lomb) has “essentially eliminated glistenings in its hydrophobic material.”
“I don’t see any downside of anyone getting a hydrophobic lens, especially with the newer materials,” Dr. Gorovoy said.
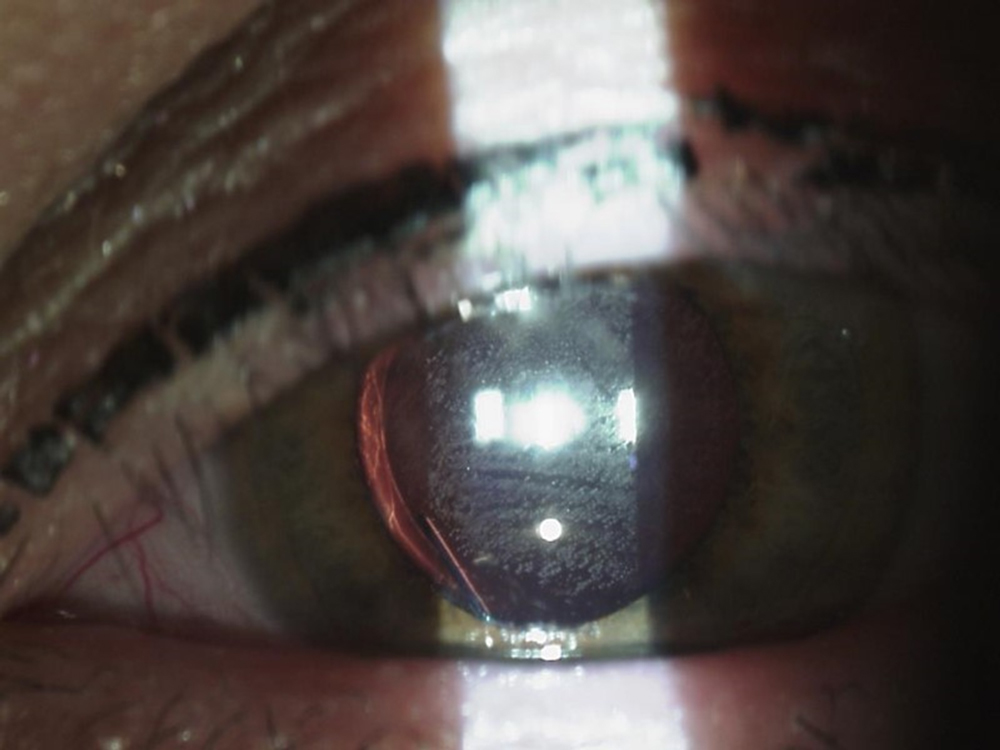
Source: Mark Gorovoy, MD
Hydrophilic acrylic
Dr. Wortz said he has performed about 35,000 cataract surgeries, most of which have been with hydrophilic acrylic IOLs.
“The thing I like about hydrophilic acrylic is I think it does have a lower index of refraction. It’s a bit thicker, and even though it does tend to have a bit more PCO, I can deal with PCO with the YAG laser. I can’t as easily deal with some of the other things like reflections or negative dysphotopsia with a YAG,” he said. “If there’s a problem that I can solve noninvasively, I think that’s better. So hydrophilic is, in my opinion, equally as good of a material and in some ways better than hydrophobic, with one exception.”
This exception, he said, is a patient with Fuchs endothelial dystrophy who ends up needing a DMEK with an air bubble, which, as Dr. Gorovoy and Dr. McKee noted above, can lead to calcification and opacification of the lens. Dr. Wortz said he has only seen this a couple of times in his career.
Dr. Gorovoy, in addition to not implanting hydrophilic lenses for risk of calcification, said he doesn’t think they adhere as much to the capsule, which could lead to lens decentration or secondary cataracts. Positives of hydrophilic lenses, Dr. Gorovoy said, are that they can be inserted through a small incision, they open faster than hydrophobic lenses, and they’re clear initially.
Other materials
Dr. Wortz called silicone the most biocompatible IOL material. He noted the lower risk of PCO and fibrosis with silicone but acknowledged the bad reputation the material might have gotten due to patients who later need a retinal attachment repair with silicone oil. He called these cases very rare.
“I think it ended up creating a marketing problem around a very niche, real problem,” Dr. Wortz said. “But I think silicone is a fantastic material. One of the more recently approved IOLs, the Light Adjustable Lens [LAL, RxSight], is made out of silicone.”
Dr. McKee called silicone one of his favorite materials, which he said is versatile for sulcus or capsule placement. “It always comes in a 3-piece configuration, which I prefer. The rounded edges do not cause UGH syndrome and tend to reduce dysphotopsia,” he said.
Dr. McKee also acknowledged that this material should not be used in cases where silicone oil is present or likely to be used. There have been case reports of calcification of silicone IOLs in the setting of asteroid hyalosis with an open capsule, so he may avoid this IOL material in those cases as well.
“I think the LAL is rekindling interest in silicone-based IOLs due to the outstanding refractive results achievable with this adjustable IOL,” Dr. McKee said.
Dr. McKee also gave his thoughts on PMMA and collamer materials. For PMMA, he said they are generally well tolerated, have excellent optics, and remain clear for decades. Downsides he noted include rare reports of snowflake degeneration and the larger incision sizes required for these non-foldable lenses.
Collamer, Dr. McKee continued, is also well tolerated with low adverse side effects. The phakic ICL (EVO, STAAR Surgical) is the only one currently using this material, but Dr. McKee said previously available STAAR collamer IOLs were “nice options” (excluding the polyimide haptic material, which is now known to degrade and shatter over time).
What’s next
McKee said there have been good improvements in the IOL material scene in recent years. At this point, he said most IOL research is focused on creating a functional and predictable accommodating IOL. This technology will require a highly flexible material, like silicone or collamer. “Innovation in IOL material is likely to move toward improving accommodation function in the future,” he said.
Dr. Gorovoy said he’s happy with IOL materials at this point but would like to see new designs, specifically those that reduce or eliminate dysphotopsias. He would also like to see better three-piece lenses for scleral fixation, as well as piggyback lenses.
Dr. Wortz’s wish list also wasn’t necessarily for better materials, but he said he would like to see lenses with larger optics for patients with larger pupils, a true accommodating IOL, and anything that’s more biocompatible that reduces or eliminates PCO. Additionally, future IOL platforms need to be designed on an exchangeable platform. “Since no material is perfect, and we cannot predict the future pathology of the eye or what a patient will tolerate, I think we need to have a better backup plan for IOL exchanges of all lenses regardless of material. We should not risk damaging the bag or zonules in order to remove an optic that is not functioning for a patient,” he said.
ARTICLE SIDEBAR
Definitions
Dr. McKee said to really understand IOL materials, it’s important to understand the definitions of the common attributes that determine their behavior. Here’s how Dr. McKee described the following terms.
Abbe number: This measures the degree of chromatic aberration of a lens (change of refractive index vs. wavelength). The human eye cannot detect chromatic aberration in a lens if the Abbe number is above 40. The crystalline lens typically has an Abbe number around 45.
Asphericity: This measures deviation from a perfect sphere, expressed as the Q value. Negative Q values indicate a prolate lens; positive Q values indicate an oblate lens. Aspheric IOLs can alter spherical aberration, which can affect contrast sensitivity vs. depth of field. In ophthalmology, Q factor typically refers to the corneal asphericity. Considering corneal Q factor, an IOL can be chosen to minimize spherical aberration to increase contrast sensitivity or allow for a small amount of spherical aberration to increase depth of field at minimal expense to contrast sensitivity.
Hygroscopy: This is the propensity of a material to adsorb water. Hydrophobic IOLs with low hygroscopy tend to form glistenings.
Glass transition temperature (Tg): This is the temperature at which a polymer changes from a rigid (glassy) state to a flexible state. A high Tg results in a non-foldable IOL (PMMA). Foldable IOLs do not unfold easily below their Tg. The lowest Tg and thus fastest unfolding IOL material is silicone.
Refractive index: Higher refractive index IOLs can be thinner but may also have more surface reflection and dysphotopsias (hydrophobic acrylic). Lower refractive index IOLs may have less of these problems but are thicker and may require a larger incision size (silicone).
“Ideally, we want an IOL that is foldable for reducing incision size, optically clear with minimal chromatic dispersion (high Abbe number), a refractive index near the natural lens (1.4, to prevent reflections and dysphotopsias), the largest optical zone, the lowest incidence of dysphotopsias, the highest biocompatibility, and that does not opacify under any conditions in the eye. This is asking a lot, but I think we are fairly close to that ideal material.”
About the physicians
Mark Gorovoy, MD
Gorovoy M.D. Eye Specialists
Fort Myers, Florida
Yuri McKee, MD
East Valley Ophthalmology
Mesa, Arizona
Gary Wortz, MD
Commonwealth Eye Surgery
Lexington, Kentucky
Relevant disclosures
Gorovoy: None
McKee: Bausch + Lomb, Haag Streit, JelliSee, Zeiss
Wortz: Alcon, Bausch + Lomb, Johnson & Johnson, Omega Ophthalmics, Rayner
Contact
Gorovoy: mgorovoy@gorovoyeye.com
McKee: mckeeonline@mac.com
Wortz: 2020md@gmail.com