Cornea
Spring 2025
by Ellen Stodola
Editorial Co-Director
Opacified corneas can present an additional challenge when preparing a patient for cataract surgery. Several physicians discussed how they handle these patients and specific considerations.
The challenge when someone has a cornea that’s opacified and there is a cataract is determining how much of the problem is the cornea and how much is the cataract, said Kevin M. Miller, MD. Sometimes you don’t know, he said, adding that the order or whether you deal with both issues at the same time is important, especially to the patient. “You don’t want to do more surgery than you have to, and a general rule of thumb is that patients like to keep their own corneal tissue and not get someone else’s.”

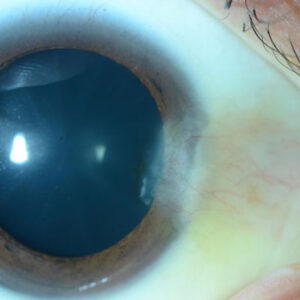
Source: David R. Hardten, MD
When Dr. Miller sees a patient with an opacified cornea, he finds out if it’s a stationary problem or if it’s going to progress. If it’s progressive, it’s going to be like Fuchs dystrophy or bullous keratopathy. Cataract surgery will be another ding to help it progress and set the cornea further behind. If it’s stationary, you must determine if the patient will see relatively well through the clear parts of the cornea if you leave the cornea alone and only take out the cataract.
“That’s a judgment call, and it’s based primarily on where the opacity is with respect to the pupil,” he said. If the vision is going to be limited and you don’t want to subject the patient to a lot of additional risk, Dr. Miller said he generally takes out the cataract first if the cornea is stable. However, he noted that sometimes it’s necessary to address the cornea first.
The advantage of doing the cornea procedure first is it stabilizes the overall situation, and you can often get a better refractive result when you perform the cataract surgery, especially if you use the Light Adjustable Lens (LAL, RxSight), Dr. Miller said. “But the problem with doing it in that order is that when performing the cataract procedure, you’ll damage the cornea with the trauma and inflammation.”
If the patient has a stable corneal opacity not immediately blocking the pupil, usually the best thing to do is take out the cataract and see how they do, Dr. Miller said, suggesting that you might want to give them a few months to a year, and if they’re still having problems, handle the cornea issue. The LAL works well if you’ve done a corneal transplant and it’s clear, he said. The problem would be if you have a corneal scar, you don’t want to use an LAL because UV light won’t get through the scar.

Source: Kevin M. Miller, MD
David R. Hardten, MD, said that if the cornea is the main issue for vision problems, he likes to try to sort that out first or at the same time as the cataract surgery. A common condition is Fuchs dystrophy, where a DMEK and cataract surgery combined is a common plan, he said. If the patient has a significant scar where the view is impossible, with a moderate cataract he will do a corneal transplant first and perform the cataract surgery several years later when the corneal curvature is stable.
Zeba A. Syed, MD, said that slit lamp evaluation prior to cataract surgery will generally reveal clues as to what is causing the opacified cornea. “During preoperative evaluation, it is crucial that the clinician obtain additional history or testing to ascertain possible underlying etiologies for the corneal opacification,” she said. “Specifically, the surgeon should identify the chronology of the opacification, progression, and history of prior infection. Diagnostic procedures that may be performed include topography, tomography, pachymetry, specular microscopy, and anterior segment OCT.”
Dr. Syed also noted that corneal opacification may be due to a number of etiologies. “Prior infection is a common cause of corneal scarring. While bacterial keratitis is common, the surgeon must also consider the possibility of herpetic infection because viral reactivation is a concern after intraocular surgery. In these latter cases, prophylactic antiviral in the perioperative period should be considered,” she said. Keratoconus is another common cause of cornea scarring, often in those with prior hydrops, and Dr. Syed said these patients may have a chronic history of poor vision or hard contact lens use.

Source: Kevin M. Miller, MD
In cases where it is hard to ascertain whether visual impairment is arising primarily from the cataract or the cornea, a hard contact lens over refraction can be performed, she said. “A careful history should be performed to understand what the patient’s vision was prior to the cataract forming but after the opacity developed, as this helps manage postoperative expectations,” Dr. Syed said. “In cases of dense corneal scarring, combined penetrating keratoplasty with cataract surgery can be considered. In younger patients, I often discuss staged penetrating keratoplasty followed by cataract surgery after topographic stabilization. When cataract surgery is performed in the presence of corneal scarring, patients can be referred for a hard contact lens fitting 4–6 weeks after cataract surgery.”
In other cases, Dr. Syed said corneal opacification may be due to underlying endothelial dysfunction, and edema with possible haze or scarring may be the primary clinical features. “Specular microscopy should be performed bilaterally to determine endothelial cell density, and pachymetry should be obtained to determine corneal thickness,” she said. “Patients should be counseled on the risk of further endothelial decompensation after cataract surgery. In severe cases, combined endothelial keratoplasty with cataract surgery may be considered. Staged endothelial keratoplasty followed by cataract surgery after the cornea clears is also a possibility and should be considered in patients with unreliable keratometry values or in those with greater refractive demands.”
Intraoperative visibility is the primary concern when performing cataract surgery under an opacified cornea, Dr. Syed said. “With poor visibility, surgical complications, such as capsular tears, are more likely. Depending on the underlying etiology of the opacity, various approaches may be taken to improve visibility prior to surgery. In the case of superficial stromal scars, superficial keratectomy with PTK laser may be an option, she added.
“I perform an anterior segment OCT to measure the depth of pathology and to plan my PTK treatment,” Dr. Syed said. “The benefit of this approach is that it can, in a fairly predictable way, laser away the scarring while leaving the cornea smooth enough for reliable keratometry and predictable refractive outcomes. If this approach is taken, I typically wait about 3 months before repeating biometry for cataract surgery.”
When considering the challenge of intraoperative visibility, Dr. Syed said there are various tools to help overcome this. The light microscope’s settings can be tweaked to improve the red reflex, which can be extremely helpful during capsulorhexis construction, she said. “I often use capsular staining with trypan blue to help enhance visibility of the capsule while performing a capsulorhexis. A light pipe can effectively improve intraocular visibility during surgery without a clear cornea.”
Dr. Miller also highlighted some considerations during surgery in these cases. If the corneal problem is progressive, like endothelial failure, the cataract operation is going to make that problem even worse, he said. “We do everything we can to reduce trauma to the endothelium,” he said. “That means using plenty of dispersive viscoelastic, replacing it as often as you need to.” If it’s a stromal scar but the endothelium is fine, you can do standard cataract surgery, but you might have to move the eye around during surgery so you’re viewing through a part of the cornea that’s clear. Often, it can help to use dyes like trypan blue to enhance contrast.
Dr. Miller said it’s not ideal to use multifocals, EDOF lenses, or toric lenses if the cornea is irregular. If there’s any chance a patient is going to need a rigid contact lens to even out the cornea irregularity, the last thing you want to do is implant a toric lens, he said. “A general rule of thumb for bad corneas is to go for simple lenses,” Dr. Miller said, with the exception of the LAL being an option as long as there’s no corneal opacity.
Dr. Hardten likes to use trypan blue for capsular staining when the view is marginal, and he said this helps avoid the anterior capsular rim with the phaco tip and aids in lens placement in the capsular bag. Newer microscopes help with better red reflex and visualization.
“I typically use my usual monofocal IOL for these cases,” he said, agreeing with Dr. Miller that you should avoid toric or multifocal when there is significant corneal opacity or irregular astigmatism. Dr. Hardten said that many of these patients can benefit from a scleral lens a few weeks after the cataract surgery. If the patient still has inadequate vision, another discussion on corneal transplant or PTK could be had, he said.
For postop considerations, Dr. Miller said this gets back to the initial discussion of whether the problem in the cornea is stationary or progressive. If it’s stationary, you do routine postop care, and if vision is reasonably good, have the patient come back in a year. With a progressive condition and cornea/endothelial failure, you must keep watching the patient. If they progress to endothelial failure, you’ll have to manage it. If they don’t fail, they may have to wear glasses for watching TV or driving if you targeted mild myopia, but if they do, they’ll have been set up nicely for a corneal transplant. He added that for patients in whom a corneal transplant is likely, he’ll overpower the lens to leave the patient a little myopic because an endothelial keratoplasty will push them in a hyperopic direction.
Dr. Syed said that if there is significant corneal scarring that extends to the peripheral cornea, the stroma often loses its sponginess, and incisions may not self-seal as they would normally. “I typically have 10-0 nylon sutures on standby in case sutures are needed to seal the incisions. If the opacity is due to a herpetic etiology, viral reactivation is a possibility, and the patient should be monitored closely for any flare-ups while on antiviral prophylaxis,” she said. “Given that the intraoperative view was likely inadequate, there may also be small, retained lens fragments present postoperatively that were not removed entirely during surgery and may cause prolonged inflammation.”
Dr. Syed finds that preoperative counseling is key. In patients undergoing cataract surgery with an opacified cornea, the surgeon should explain beforehand that the cornea and not just the cataract is playing a role in their visual symptoms. While some visual improvement is expected, the final vision will be limited to some degree by the opacified cornea.
Dealing with corneal opacities is common in a typical practice, Dr. Miller said. A lot of patients get corneal ulcers or trauma to the eye, and you see these patients many times a year. Most people have developed their own little tricks to manage them, he added.
About the physicians
David R. Hardten, MD
Attending Surgeon
Minnesota Eye Consultants
Minnetonka, Minnesota
Kevin M. Miller, MD
Kolokotrones Chair in Ophthalmology
David Geffen School of Medicine at UCLA
Los Angeles, California
Zeba A. Syed, MD
Director of the Cornea Fellowship Program
Associate Professor of Ophthalmology
Wills Eye Hospital
Philadelphia, Pennsylvania
Relevant disclosures
Hardten: None
Miller: None
Syed: None
Contact
Hardten: drhardten@mneye.com
Miller: kmiller@ucla.edu
Syed: zsyed@willseye.org