Refractive: Evolving
Winter 2024
by Ellen Stodola
Editorial Co-Director
With expanding options in refractive surgery for patients at different ages, many physicians are seeing an uptick in refractive lens exchange (RLE). Marjan Farid, MD, D. Rex Hamilton, MD, and Luke Rebenitsch, MD, discussed their experience with RLE, including considerations when explaining this option to patients.
The average age of cataract surgery in this country has come down with advancing technologies and the ability to restore vision with advanced-optic IOLs, Dr. Farid said.
“We have a lot of patients who come in who are pre-cataract and very frustrated with their vision and spectacle and contact lens requirements and want refractive solutions,” she said. “The whole arena of refractive surgery has expanded beyond LASIK, with phakic IOLs, SMILE, PRK. Patients come in and ask if they’re a candidate for LASIK because they don’t want to wear glasses anymore, and in a certain population of patients, refractive lens exchange is a much better solution.”
Source: D. Rex Hamilton, MD
Dr. Farid said patients who are presbyopic, between the ages of 40–60, may not be the best candidates for LASIK because that will keep them in glasses for certain activities. Other patients who are great candidates for refractive lens exchange are younger patients who are very hyperopic; hyperopic LASIK is less predictable, even with available nomograms, Dr. Farid said. Patients with higher hyperopia have smaller eyes and are at risk for future narrow angle-related glaucoma. “We have 40-year-olds coming in who have been told they have narrow angles and might need laser peripheral iridectomy and are high hyperopes where laser peripheral iridectomy is temporary. [RLE] is a refractive solution because these patients often have poor vision and need coke bottle spectacles or contact lenses.”
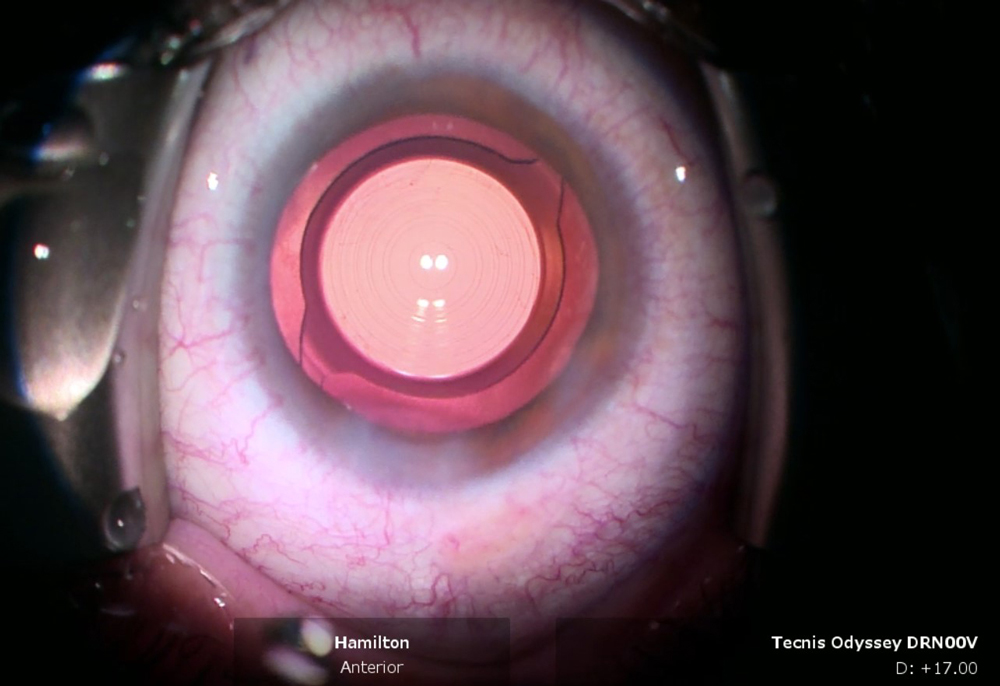
Given that RLE patients generally want spectacle independence, Dr. Farid considers advanced-technology IOLs for them first. She particularly likes the TECNIS Odyssey IOL (Johnson & Johnson Vision) and the Light Adjustable Lens (LAL, RxSight).
The TECNIS Odyssey, she said, is more of a full range of vision lens, and patients have been blown away by its optical quality and enhanced contrast sensitivity. There is a free-form technology on the optic that minimizes the side effects of glare and starbursts, so these patients have minimal complaints of nighttime dysphotopsias, and they get good range of vision.
Source: D. Rex Hamilton, MD
“The other one I love is the LAL+ for patients because they come out of surgery already with some range of vision, then we can build in a little more with adjustments postoperatively, and this is another lens that gives great quality of vision,” she said.
Dr. Hamilton said he frequently sees patients who want to get out of their glasses and tell him they want LASIK. “That might work for someone in their 20s–30s, or even into their 40s, but if someone in their 50s comes in, and they’ve never worn glasses before and are having trouble seeing up close, but they want LASIK, I say, ‘LASIK is done on the cornea. The reason you’re having trouble at 50 is not due to the cornea but rather the lens inside, which loses its flexibility and doesn’t focus as well. It will become cloudy in the future as a cataract develops. A cataract is not a disease but part of the aging process. With RLE, we are preventing cataract formation and restoring vision from distance all the way to the cellphone without glasses.’”
Dr. Hamilton’s practice website has a section that discusses options for patients at various ages. The under 40 page has information on LASIK, SMILE, and the EVO (STAAR Surgical), while the over 50 page discusses options like RLE, laser cataract surgery, and the LAL but does not include LASIK. Patients in their 40s–50s require individualized care.
Some of the most ideal patients for RLE, he said, are the hyperopes because they were used to not wearing glasses and now are dependent on them at least for near vision and often for distance. They are delighted to get back the unaided near and distance vision.

Source: Jaire Zaleta, ClearSight
“One of the reasons why I am much more enthusiastic about RLE now is because we have amazing lens implants,” Dr. Hamilton said, adding that he is also excited about the TECNIS Odyssey, which he called “incredible in terms of distance, intermediate, near, and minimizing nighttime halos.” For patients in their 40s and early 50s, quality of vision is still quite good because there is not much nuclear sclerosis. Therefore, they are expecting not to lose this quality with RLE. Some of the multifocal lenses have contrast sensitivity issues that may not be acceptable to patients in their 40s and early 50s from a quality of vision standpoint. “I have not found that to be the case with the TECNIS Odyssey,” he said, noting that this lens is only available in a limited market release right now, but he has been using it since April 2024. “It has been transformational to me in terms of RLE.”
Dr. Hamilton also likes to use the LAL in patients who have had previous refractive surgery. “The best patients are the ones who have had previous hyperopic LASIK and patients with smaller pupils,” he said. “They get amazing results from the LAL. The patients who don’t get as much range are the ones with big myopic corrections and larger pupils.”
The LAL is still a great choice for post-LASIK patients with myopic corrections, but you have to set the expectations, he said. It’s going to be blended vision; the two eyes will be different. The patient will decide how much near vision they want in exchange for distance quality.
The myopes are a different breed from hyperopes. They come in because they’re taking glasses off to read for the first time, Dr. Hamilton said. “If someone in their late 30s or early 40s comes in with a –7 and I do LASIK on them, it changes corneal optics in a negative way. I’m going to create too much positive spherical aberration. Now in 5–6 years, they’ll come back and say the LASIK wore off, but I’m going to say that we talked about that LASIK is not the final solution. I won’t have as many options for that patient because we did LASIK and created optics not compatible with some options, like the multifocal lens. This is another reason why I’m not doing LASIK in patients with high myopic corrections in their late 30s and early 40s.” For these patients Dr. Hamilton prefers to use the EVO. “I can put the EVO in, I haven’t altered the corneal optics, and when they come back in 5–10 years for RLE, we have more options available,” he said.
Dr. Rebenitsch said the best education happens even before patients come through the door. “It’s important to have this information on your website and in marketing materials that there are solutions beyond LASIK,” he said.
In terms of RLE candidacy, Dr. Rebenitsch said it’s the same evaluation for cataract surgery for candidacy for multifocals. The technology, he continued, is even more important in RLE because this is elective surgery. “The expectations are higher with RLE than with refractive cataract surgery, so it’s important to not only have the conversation about what it’s going to take to adapt, … but it’s also important to talk about what happens if they need a touchup or what it will look like in the future.
“Two of the newest players are the TECNIS Odyssey and the Lenstec ClearView 3 segmented bifocal,” Dr. Rebenitsch said. “We found that for those who are concerned about glare and halo, they tend to be less.” He’s finding success with these lenses in virgin corneas and post-refractive eyes.
Preop testing and evaluation
In terms of preoperative testing and evaluation, it’s similar to refractive cataract surgery. “You want a good topography, you want to look at the mires, you want to look for dry eye,” Dr. Rebenitsch said.
Dr. Rebenitsch likes to use the OPD-Scan III (Marco). He also noted tests for tear osmolarity and looking at overall higher order aberrations (HOAs). Just like cataract surgery, it’s important to look at the macula for signs of ERM, PVD (if there’s not one yet, there’s a decent chance it could induce PVD), he said.
Dr. Hamilton said there are several considerations. On the myopic side, we want to have a good retina exam, he said. We also want to have a discussion with the patient about the risk of retinal tears and detachments. “I would insist that myopic patients get plugged in with a retina specialist and go for dilated exams periodically for a few years after RLE.” The PVD is critical because the presence of a complete PVD drastically reduces the risk of retinal tear and detachment. Unfortunately, we don’t have great imaging for PVDs, he said. “We can see if the vitreous is still attached in most situations; it’s hard to know if it’s totally detached, so that’s an area where we need better imaging.”
Enhancement plan
Dr. Hamilton said that in virgin eyes, modern formulas are remarkably accurate. He added that if you’re going to do a lot of RLE, you have to be comfortable with IOL exchange. “For the post-refractive patient, we’re using the LAL primarily, and it’s essentially a non-issue because you can adjust the power after if there’s a miss.”
Dr. Rebenitsch has found the typical RLE patient rate of enhancement is about two times the rate of traditional refractive cataract surgery. It’s about setting expectations, he said, adding that he brings patients back after 3–4 months. “We run all the tests again and see if there’s anything we need to do to enhance vision further; 20/happy is what we’re going for, but it’s harder to get that with RLE.”
Especially for post-LASIK patients, Dr. Farid strongly recommends the LAL because she doesn’t want to do another LASIK or PRK enhancement on a cornea that’s already been touched. If they haven’t had LASIK, she said it depends on the type of patient and lens you go with. “If we go forward with a multifocal lens, we do talk about possibly enhancing. If it’s a virgin cornea, I’m more comfortable doing laser vision enhancement if needed.”
The ocular surface
The ocular surface is going to be a key player for any patient having refractive surgery, Dr. Farid said. Preoperatively, she will put these patients on a treatment regimen based on how dry they were before. “Sometimes I’ll be really aggressive for those who have significant dry eyes before surgery, but even if they don’t have symptoms, I still talk about dry eyes,” she said. “I talk about starting basic things like hot compresses, so the patient understands that this is something we’re going to be treating after surgery as well.”
Dr. Rebenitsch said there are different schools of thought on handling the ocular surface. If there is significant OSD present, they’ll most likely suffer for years to come, he said. Even though we can improve it, we’ll avoid a traditional diffractive multifocal and maybe even a ClearView 3 and move to an LAL or monovision, he said.
If there’s OSD in advance, you want to treat it. “With RLE, we want to know we can hit that refractive target, so we want OSD to be known in advance rather than a perceived complication in the future,” he said.
Contraindications for RLE
According to Dr. Rebenitsch, RLE should be done in two settings: if the surgeon can almost always do the procedure without complications and if there are no systemic risks. With anything that’s going to increase risk beyond baselines, we don’t do RLE, he said.
Dr. Farid said she would be cautious with RLE for patients who have very high myopia. Those patients at baseline have a higher risk of peripheral retinal tears, higher risk of detachments, more of a formed vitreous. They’re better phakic IOL candidates. “But if they really want a refractive lens exchange, those are patients who need to see their retina specialist,” she said.
Certain patient personalities may be a contraindication as well, and Dr. Farid said it’s all about setting proper expectations and patient education. “Any refractive patient needs to understand that the goal of the surgery is to decrease the dependence on glasses. I almost never say ‘completely eliminate’ the need for glasses because even with the best lenses, there are some occasions where the patient needs to wear glasses,” she said.
Dr. Hamilton said it’s important to look out for certain pathologies before performing RLE. For example, he said you wouldn’t want to put a Tecnis Odyssey or multifocal lens in someone with keratoconus. Additionally, he said it would be hard to meet expectations for those with retinal disease or diabetes.
The bigger issue, he said, is the younger patients and the quality of vision at distance and the plano presbyope. “I’ve done RLE on plano presbyopes who are in my chair because of reading glasses, doing the procedure not to get distance better but to get near vision. They assume the distance vision will be the same after RLE. I am cautious in these patients and explain they may initially be disappointed with the distance vision. If they decide not to do surgery, that’s fine. They leave understanding the natural course of vision with aging is it gets worse as presbyopia progresses and cataract develops. Patients appreciate not being pressured into surgery and come back when their vision gets worse.”
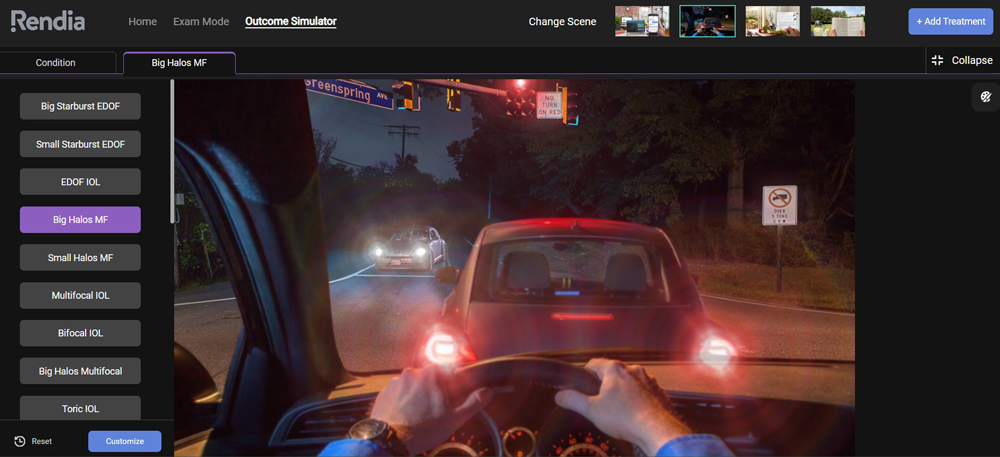
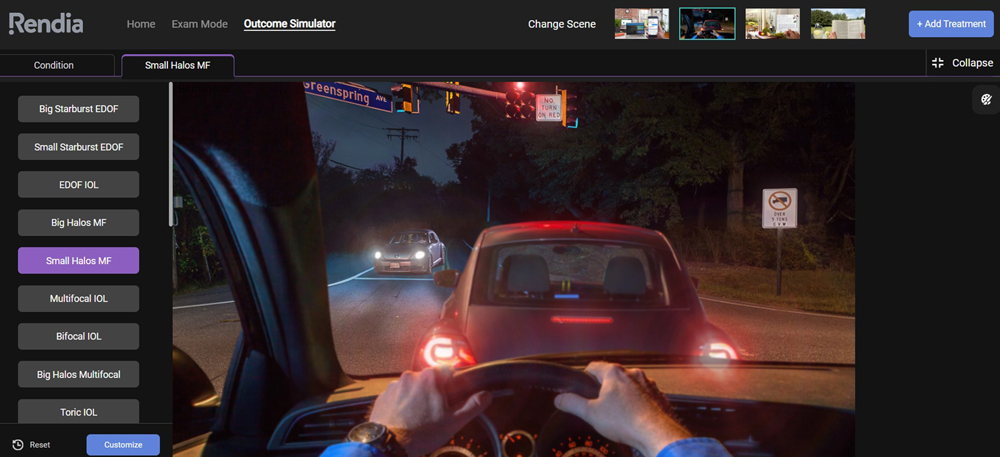
Dr. Hamilton also takes patient personalities into consideration. He uses a simulator (Rendia) to show the potential vision as well as night dysphotopsia. You must discuss nighttime issues, he said. If someone is a plano presbyope and doing this for near vision, for example, we must explain what to expect regarding quality of vision, particularly in dim light. “I tell them that they’re going to see halos; that’s how the lens works, and the brain has to adapt. Then I wait for a reaction.” He noted that the TECNIS Odyssey lens seems to have less nighttime dysphotopsia, and neuroadaptation occurs faster than with previous multifocal IOLs.
Growth in RLE
Dr. Hamilton has noticed an uptick in RLE over the last year or two and added that using the TECNIS Odyssey lens has made him even more confident with a wider range of patients.
“One of the great features about RLE is I’m doing them bilateral same day,” Dr. Hamilton said. “The primary reason we don’t do cataract surgery bilateral same day is a financial one, … but RLE is cash pay.” Patients are happy to get both eyes done at the same time. Neuroadaptation is faster, and there is no in-between time with anisometropia that can sometimes muddy the waters for the patient deciding to move on to the second eye.
Dr. Rebenitsch estimated that more than 50% of his practice revenue is from RLE. “We started doing RLE 10 years ago, and it has now grown to be bigger than our other refractive volume in terms of revenue,” he said. He estimated that he’s now doing around 1,000 RLEs per year (500 patients).
“People want it,” he said. Everyone is frustrated with readers and bifocals, and while patients have heard for many years and know about the benefits of LASIK, they often have in their mind that with LASIK they’ll have to give something up in their 40s. “That’s where RLE shines,” Dr. Rebenitsch said.
About the physicians
Marjan Farid, MD
Director of Cornea, Cataract, and Refractive Surgery
Gavin Herbert Eye Institute
University of California, Irvine
Irvine, California
D. Rex Hamilton, MD
Medical Director
Hamilton Eye Institute
Beverly Hills, California
Luke Rebenitsch, MD
Medical Director
ClearSight
Oklahoma City, Oklahoma
Relevant disclosures
Farid: Alcon, Carl Zeiss Meditec, Johnson & Johnson Vision
Hamilton: Alcon, Carl Zeiss Meditec, Johnson & Johnson Vision, RxSight
Rebenitsch: Carl Zeiss Meditec, Johnson & Johnson Vision, RxSight, STAAR Surgical
Contact
Farid: mfarid@hs.uci.edu
Hamilton: rex@rexhamiltonmd.com; rexhamiltonmd.com; hamiltonrle.com
Rebenitsch: lrebenitsch@gmail.com