Glaucoma: Strike!
Fall 2024
by Liz Hillman
Editorial Co-Director
Needling and hypotony were once more common obstacles with the XEN Gel Stent (AbbVie), however, after several years and lessons learned, many surgeons have adopted new approaches that have increased success rates and reduced the need for subsequent procedures. EyeWorld spoke with Ang Li, MD, and Jithin Yohannan, MD, to get their insights on the pearls they have gained using the stent, which originally received FDA approval in 2016.
Dr. Li said she began using the XEN early in practice, shortly after its approval. Over the years, she’s found the ideal candidate to be the elderly, Caucasian patient who may be intolerant of drops with moderate to severe glaucoma or patients in whom she is looking to avoid tube shunts or trabeculectomy.
“It’s less invasive and postoperatively more tolerated by most patients compared to tubes or trabs. I do like to use it for surgically naïve patients because it has specific requirements for conjunctiva and Tenon’s tissue, so operated-on eyes generally don’t do as well, and they scar down more easily,” she said, noting that she is usually aiming to get pressures in the mid-teens with the XEN.
Dr. Yohannan has similar criteria for XEN patient selection. He uses this stent on patients with uncontrolled glaucoma with more advanced damage whose IOPs are above target. He reserves the XEN for patients at higher risk for hypotony with a trab and those who are at less risk for bleb fibrosis. This includes older patients, high myopes, and patients who are not of African decent.
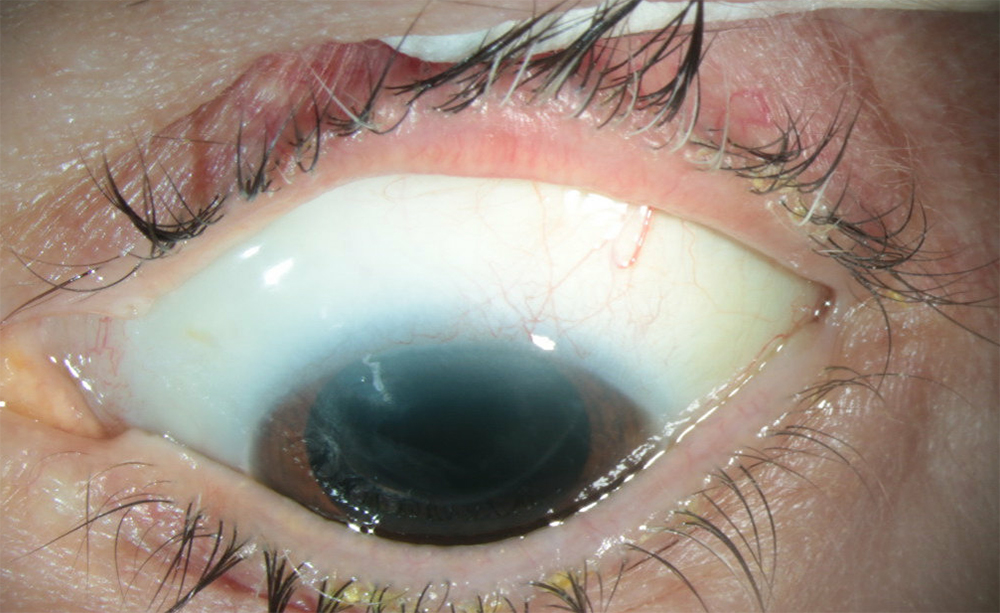
Source: Ang Li, MD
Obstacle #1: Ab interno approach
The XEN is approved for insertion in the subconjunctival space via an ab interno approach. However, Dr. Li and Dr. Yohannan—and many other glaucoma specialists—have adopted an ab externo approach for certain patients. “If you look at a random survey of glaucoma colleagues, it’s about 50/50 or even more ab externo for how physicians are using it,” Dr. Li said.
The ab externo approach’s safety and efficacy has been compared to the on-label, ab interno approach many times. In these studies the ab externo procedure was found to have at least the same efficacy and safety as the ab interno procedure—in some cases even resulting in a higher success rate.1–4
Some of the challenges of the ab interno approach are avoided when doing ab externo, Dr. Yohannan said. These include the skill required for working in the angle with a mirrored gonioprism and finding the right plane for the stent to be placed in the subconjunctival space; a higher rate of needling or the need for primary needling; a higher rate of hypotony in the postop period; and an anterior subconjunctival bleb that may be very thin and avascular and prone to leakage, XEN exposure, or bleb dysesthesia.
Dr. Yohannan said he converted to open conjunctiva, ab externo for the XEN 2–3 years ago, placing the stent sub-Tenon’s.
“I dissect into the sub-Tenon’s space. I apply high-dose mitomycin-C posteriorly in the sub-Tenon’s space (two sponges soaked with 0.4 mg/cc of mitomycin-C placed in the sub-Tenon’s space for 2 minutes and another 0.2 ml of the same concentration injected on the sponges),” he said. “I enter the anterior chamber with a 30-gauge needle. … Then I insert the stent through that 30-gauge path. There is very little flow around the stent. It’s all coming through the lumen in most cases, which I think promotes the formation of that posterior bleb. I’ll then pull Tenon’s forward, close it, and pull the conjunctiva forward and close it. The blebs that I get look much better, and the needling rate is much lower than with the ab interno approach.”
While the operative time is more for the ab externo approach, Dr. Yohannan said over the postop course, it’s better for the surgeon’s time and the patient experience than ab interno. He said it avoids the hypotony and blurry vision.
“You don’t have this anterior bleb as well, which can be more irritating to patients,” Dr. Yohannan said. “I find most patients tolerate the ab externo approach well. The surgery is more involved, but over the course of the patient’s lifetime, I would say it’s less involved. This is why I made the switch.”
Dr. Li said there are still scenarios where she thinks ab interno is warranted. These include when she is trying to conserve conjunctiva or if she’s worried about postop healing.
Obstacle #2: Needling
While the needling rate is lower with the ab externo approach, according to Dr. Li and Dr. Yohannan (in some cases, it’s difficult to even see the stent to perform needling with the sub-Tenon’s placement), lessons have been learned over the years regarding needling with the XEN.
“Initially we thought 30% of patients after the XEN needed an in-office needling, and that was a big hurdle in terms of the success and maintenance,” Dr. Li said. “More people are gravitating toward primary needling at the time of surgery prophylactically to push back the Tenon’s and prevent them from coming near the XEN. That has decreased the postoperative needling rate.”
Obstacle #3: Where to insert
Dr. Li said there is a learning curve in deciding where to insert the XEN and how to ensure it gets into the right place. “We were initially thinking it had to be subconjunctival but supra-Tenon’s, and now we’re realizing that as long as it’s not intra-Tenon’s, it’s OK. It could be sub-Tenon’s. There are various ways you can ensure that the XEN stent is in the right space. You can use an air bubble, balanced salt solution, viscoelastic, or even mitomycin-C to create a potential space for XEN insertion when doing it ab internally,” Dr. Li said.
When placing sub-Tenon’s, Dr. Yohannan said it’s important to be liberal with mitomycin- C and to ensure you don’t kink the stent when you’re closing Tenon’s.
Obstacle #4: Mitomycin-C
Since XEN’s commercial launch, Dr. Li said how the use of mitomycin-C fits into the procedure—and at what concentration—has evolved as well.
“There is still debate on that, but I think based on the patient profile, based on their surface tolerance, their Tenon’s tissue thickness, we can do a little bit more or less. There is more personalization as to how much mitomycin-C to give, and we also learned how it can affect the ocular surface under different concentrations and how to manage that postop,” she said.
Obstacle #5: Low-teens target
Dr. Li said that while she can’t count on a consistent, low-teens target with the XEN, she has had more success if she modifies the stent, cutting it to be a little shorter than its original 6 mm.
“By decreasing the length of the tube, it decreases resistance and increases the flow rate to achieve a lower IOP,” she said. “The sub-Tenon’s portion is also a little shorter so potentially you’ll have less length to be embedded into Tenon’s.”
Obstacle #6: XEN failure
Dr. Yohannan said a lot of avoiding XEN failure comes down to good intraoperative technique. If you’re placing it sub-Tenon’s, there’s not much you can do if it starts failing postop because it’s hard to needle in that position, and it’s a flimsy stent.
“It’s going to be hard to separate that thick tissue from the stent, whereas when you’re subconjunctival, it’s a little easier because there’s not thick tissue over it,” he said. “I think the main thing is ensuring you control inflammation. I’ll do steroids every 2 hours for a week. … If you have an occlusion of the proximal lumen from the iris, sometimes doing a YAG to the tip may be helpful. Even if there is no occlusion from the iris and the IOPs begin to go up, a YAG to the tip in the AC to shorten the overall length of the XEN may be helpful to increase flow and reduce IOP. In my experience, needling does not work well when the stent fails after the sub-Tenon’s approach. Most of the time, it works well with a great bleb morphology in the right patient, and you’re not subjecting them to in-office needlings.”
If the XEN fails despite these efforts, Dr. Yohannan said he’ll add back medications and see how the patient does. If they remain uncontrolled, he’ll do a trab next to the XEN. “By scarring the XEN, they’ve shown me that they’re able to fibrose well. They’re probably not going to become hypotonous after trab,” he said.
Overall, Dr. Li said, since its inception, many pearls have been learned to overcome some of the initial hurdles with the XEN. “There are so many different ways of doing the XEN, which is exciting,” she said.
About the physicians
Ang Li, MD
Assistant Professor of Ophthalmology
Case Western Research School of Medicine
Cleveland Clinic Cole Eye Institute
Cleveland, Ohio
Jithin Yohannan, MD
Boone-Pickens Assistant Professor of Ophthalmology
Johns Hopkins University School of Medicine
Wilmer Eye Institute
Baltimore, Maryland
References
- El Helwe H, et al. Comparing outcomes of 45 Xen implantation ab interno with closed conjunctiva to ab externo with open conjunctiva approaches. J Glaucoma. 2024;33:116–125.
- Tan NE, et al. Comparison of safety and efficacy between ab interno and ab externo approaches to Xen Gel Stent placement. Clin Ophthalmol. 2021;15:299–305.
- Yuan L, et al. Short-term outcomes of Xen-45 Gel Stent ab interno versus ab externo transconjunctival approaches. J Glaucoma. 2023;32:e71–79.
- Ruda RC, et al. Clinical outcomes of ab interno placement versus ab externo placement of XEN45 Gel Stents. Ophthalmol Glaucoma. 2023;6:4–10.
Relevant disclosures
Li: MicroSurgical Technology, New World Medical, Nova Eye Medical
Yohannan: AbbVie, Alcon
Contact
Li: lia2@ccf.org
Yohannan: jyohann1@jhmi.edu