Cornea: Strike!
Fall 2024
by Ellen Stodola
Editorial Co-Director
When planning cataract surgery, it’s important to pay particular attention to patients who may have a compromised cornea or endothelial damage. Francis Price Jr., MD, and Zeba A. Syed, MD, spoke with EyeWorld about considerations for cataract surgery in these eyes.
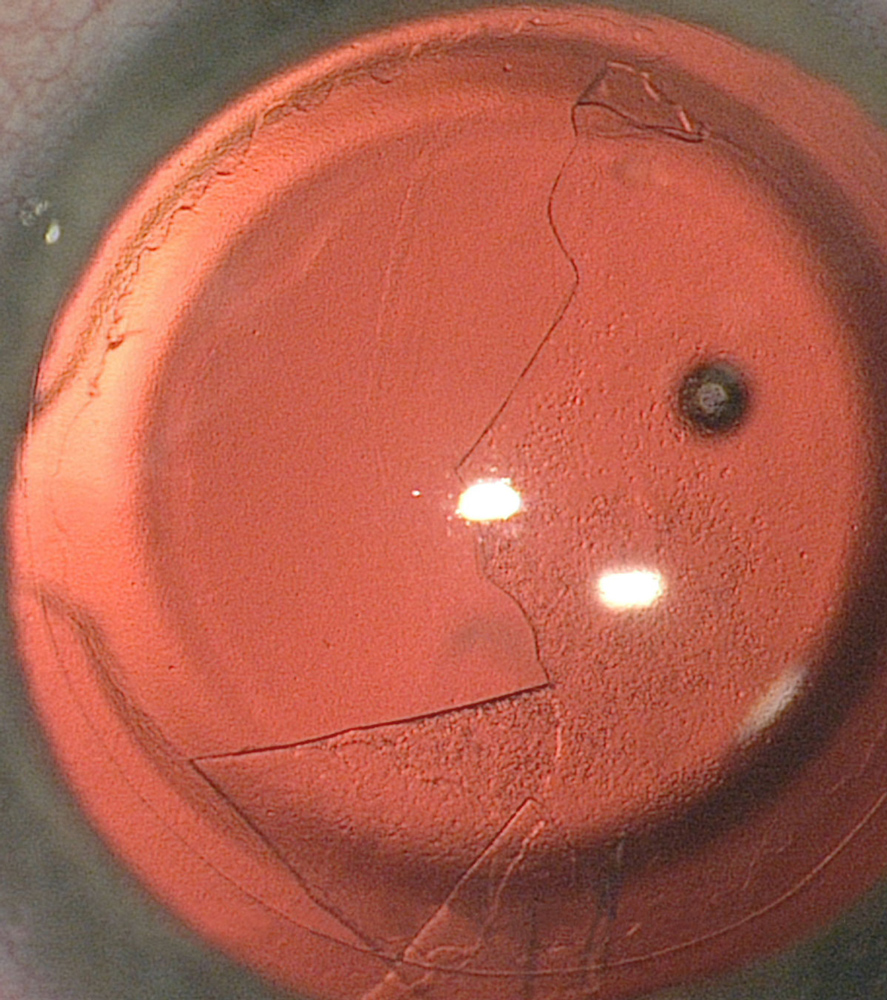
Source: Francis Price Jr., MD
“We have a lot of patients who have already compromised corneas, and the two biggest groups are those with Fuchs dystrophy and those with previous transplants, penetrating grafts, or endothelial keratoplasties,” Dr. Price said. “We know the cells naturally die off quicker in an eye that’s had a transplant than in a normal eye, so eyes with a previous transplant typically have lower cell counts. We also know that after cataract surgery in general, people lose cells more quickly than they did before they were operated on.”
While phacoemulsification techniques have improved significantly, trauma to the corneal endothelium still may occur, Dr. Syed said. This is especially important in patients with preexisting corneal compromise who have a reduced endothelial reserve. Although corneal edema is typically transient after uncomplicated cataract surgery, edema may be chronic with worsening vision.
A common risk factor for compromised corneal endothelium is Fuchs dystrophy, a disorder of guttae formation in Descemet’s membrane and endothelial dysfunction, Dr. Syed said. The ensuing corneal edema results in decreased vision with diurnal variation, and pain may also develop in advanced cases with superficial bullae formation. A study found that among patients with Fuchs who had cataract surgery, approximately 10% eventually underwent endothelial keratoplasty.1
Another risk factor for postoperative corneal edema after cataract surgery is a history of endothelial trauma. Prior glaucoma surgery, including trabeculectomy or tube placement, may have associated endothelial compromise, she said. Possible mechanisms of endothelial cell loss include altered circulation patterns of aqueous humor, intermittent tube-cornea touch, or elevated oxidative and inflammatory markers.2 Along similar lines, chronic inflammation in patients with a history of anterior uveitis can impact endothelial cell health.3
When evaluating patients preoperatively, Dr. Syed said certain features forecast further endothelial decompensation after cataract surgery. Preoperative microcystic edema, stromal thickening on the slit lamp, low central endothelial cell density (<1,000 cells/mm2), and/or increased central corneal thickness (>640 microns) predict deteriorating postoperative endothelial function.4

Source: Matt Feng, MD
Dr. Syed said that some intraoperative variables that may aggravate endothelial cell loss include the length of surgery, inappropriate use of instruments, excessive phacoemulsification energy, toxicity from intracameral medications, vitreous loss, and IOL endothelial touch. Phacoemulsification may damage endothelial cells by the production of free radicals,5 and patients with compromised endothelium are vulnerable to potentially detrimental effects.
“Strategies to reduce the risk of endothelial damage during cataract surgery include use of technology such as femtosecond lasers that may reduce phacoemulsification energy requirements, increased use of mechanical chopping, or frequent reapplication of viscoelastic to protect the corneal endothelium from phacoemulsification energy.”
Dr. Price said one of the basic things physicians can do is manage viscoelastic. He prefers the softshell technique, where you lightly fill the anterior chamber with a dispersive viscoelastic. Then you go in with a little bit of cohesive viscoelastic and put it on top of the lens, and that helps the iris not to prolapse during hydrodissection and hydrodelineation, he said. If it’s all dispersive, it can build up the pressure, and you could pop the iris out.
The other thing you need to be careful with, Dr. Price said, are shallow anterior chambers because there’s not as much working space. You want to carry out the surgery keeping the phaco as much as you can in the posterior chamber and not the anterior chamber, he said.
With a dense nucleus requiring extra energy, consider reapplying a dispersive viscoelastic a few times to protect the cornea, Dr. Price said.
You might even want to consider a different approach to cataract surgery if the nucleus is dense. While not commonly done in the U.S., Dr. Price said, for a rock-hard cataract, you might consider using manual small incision surgery, which includes making a 7–8 mm incision and expressing the nucleus manually.
After surgery, for those with endothelial damage and/or cell loss, Dr. Price said it’s important to treat the inflammation to try to minimize the amount of damage. At this point, there isn’t anything to inject to help cells regenerate, but there are a number of medicines being looked at that may stimulate endothelial cells to recover better. Dr. Price said his course of action is to increase steroids to decrease inflammation in the eye and use hyperosmotics, like sodium chloride ointments and drops, to pull out excess fluid while the remaining endothelial cells cover areas that were damaged.
We know from Descemet’s stripping only (DSO) that you can remove central Descemet’s membrane and endothelial cells, and peripheral endothelial cells will migrate over time and cover the denuded area, he said. After cataract surgery, you’ll see this around the wound, and those damaged areas usually clear up in days to weeks after endothelial cells cover areas that were damaged.
When evaluating corneal edema after cataract surgery, Dr. Syed measures central corneal thickness with a pachymeter at the first postoperative visit to record a baseline against which to compare follow-up evaluations. “While specular microscopy may be helpful in confirming endothelial cell loss, I do not always find it helpful in the setting of significant corneal edema because the measurements are often unreliable,” she said. “Another test I may use is anterior segment optical coherence tomography (AS-OCT), especially in cases where the edema may be focal. I have evaluated cases of persistent postoperative corneal edema that were actually Descemet’s membrane detachments that we identified on AS-OCT, and these cleared up with placement of an air bubble in the anterior chamber and face-up positioning by the patient. Identification of this diagnosis may prevent the patient from undergoing an unnecessary corneal transplant.”
When managing postoperative corneal edema, Dr. Syed keeps two goals in mind. The first is to eliminate aggravators of endothelial compromise, and the second is to treat corneal edema itself. In cases of immediate postoperative corneal edema, Dr. Syed said inflammation from surgical trauma often contributes to endothelial dysfunction. Topical steroids reduce inflammation as well as corneal edema in these situations.
In the presence of a quiet eye, a steroid does not usually provide any direct benefit, instead causing side effects such as increased intraocular pressure. Another approach to medical management includes hypertonic saline, which accelerates corneal deturgescence. This treatment does not directly promote endothelial viability, she said, but rather provides symptomatic relief. Hypertonic saline works well in mild edema but not as well in advanced cases. Patients should be counseled on the likelihood of long-term hypertonic saline therapy if the goal is to avoid endothelial keratoplasty.
Dr. Syed noted that rho kinase (ROCK) inhibitors are an alternative approach to manage postoperative corneal edema. The ROCK pathway plays a role in regulating endothelial cell migration, proliferation, and adhesion, and ROCK inhibitors support endothelial wound healing and accelerate corneal deturgescence after surgery.6 Options for ROCK inhibition include netarsudil 0.02% and ripasudil 0.4%. Both formulations may improve endothelial cell viability after surgical trauma. “I typically use the ROCK inhibitor 4 times daily for 4–6 weeks postoperatively or until corneal deturgescence is noted, although I will titrate based on tolerability,” she said.
If edema persists a couple of months out, Dr. Price said there’s a good chance it’s not going to clear and to consider an endothelial keratoplasty. For a non-Fuchs patient, he’ll do cataract surgery alone when there’s a low cell count because if you use a good technique, the patient can maintain a low cell count for years with or without a previous graft.
Fuchs is a different story. The guttae affect vision, he said. “I operate on people with no apparent edema but who have guttae causing glare and haze, and we see improvements for those patients.” If they have guttae and a cataract, Dr. Price recommends treating both at the same time. Patients can have some improvement from just treating the cataract, but often, that may lead to corneal decompensation.
When explaining guttae to patients, Dr. Price likens them to raindrops on a windshield. A few scattered guttae don’t noticeably degrade vision, but as you get more, they start to affect vision. Like raindrops, guttae cause light scattering. If there are significant guttae over the pupillary area, he’ll typically do a combined case with cataract and DMEK, Dr. Price said. “That said, it’s harder to hit the refractive target with the IOL because the guttae and clinically evident or sub-clinical edema associated with Fuchs dystrophy throw off the accuracy of biometry. Even when preoperative corneal edema is not discernible by slit lamp exam, we notice that the central corneal thickness usually decreases after DMEK in eyes with Fuchs dystrophy, and those changes affect the refractive accuracy,” he said.
Dr. Price recommends three options to patients with cataracts and Fuchs:
- Do a combined case with a standard monofocal lens. Most patients do well, but the final postoperative spherical equivalent can range –2 to +3 D from the target, and that’s a big range because with standard cataract surgery, most fall within ±0.5 D of the target. A high degree of refractive accuracy is required for satisfactory use of a multifocal IOL, so these are contraindicated in combined procedures.7
- For patients who want a multifocal lens and have cataract and Fuchs, Dr. Price will do DMEK first and put the multifocal lens in 2–3 months later. With this staged approach, you need to do the cataract second because if you do the cataract first, the patient will still have irregularity from Fuchs that throws off the biometry used to select the IOL power.8
- The last option he mentioned was DMEK combined with implantation of a Light Adjustable Lens (LAL, RxSight). The LAL is approved for 2 D of postoperative adjustment, so that almost covers the range of error, Dr. Price said. It gives you a good chance of getting most patients close to plano. He uses the LAL for a quarter of patients in whom he does combined cases and has published on this approach.9 It takes longer for refractions to stabilize after DMEK than after standard cataract surgery, so he is slower to proceed with lens adjustment and lock-in after combined procedures.
In cases of visually significant cataract with moderate to severe Fuchs or with significant corneal edema, Dr. Syed said she often combines cataract surgery with an endothelial keratoplasty. “The benefit of this approach is that it saves the patient from requiring a second surgery.” Intraoperatively, these cases may be challenging due to reduced visualization through an edematous cornea. “I find epithelial debridement to improve the view significantly in cases of epithelial edema,” Dr. Syed said. “Keratometry changes after endothelial keratoplasty can be highly unpredictable, particularly in those with superficial edema. Hence, I counsel these patients on the likely need for spectacle correction after combined endothelial keratoplasty and cataract surgery.”
Dr. Syed will also use staged endothelial keratoplasty followed by cataract surgery, particularly when patients have higher refractive expectations or needs. “This approach is helpful in individuals who desire a toric or presbyopia- correcting IOL,” she said. “Of course, the risk in this case is further endothelial cell loss in the graft secondary to cataract surgery.”
About the physicians
Francis Price Jr., MD
Price Vision Group
Indianapolis, Indiana
Zeba A. Syed, MD
Director
Cornea Fellowship Program
Wills Eye Hospital
Philadelphia, Pennsylvania
References
- Das AV, Chaurasia S. Clinical profile and demographic distribution of Fuchs’ endothelial dystrophy: An electronic medical record-driven big data analytics from an eye care network in India. Indian J Ophthalmol. 2022;70:2415–2420.
- Vallabh NA, et al. Corneal endothelial cell loss in glaucoma and glaucoma surgery and the utility of management with Descemet membrane endothelial keratoplasty (DMEK). J Ophthalmol. 2022;2022:1315299.
- Alfawaz AM, et al. Corneal endothelium in patients with anterior uveitis. Ophthalmology. 2016;123:1637–1645.
- Kaup S, Pandey SK. Cataract surgery in patients with Fuchs’ endothelial corneal dystrophy. Community Eye Health. 2019;31:86–87.
- Sharma N, et al. Corneal edema after phacoemulsification. Indian J Ophthalmol. 2017;65:1381–1389.
- Antonini M, et al. Rho-associated kinase inhibitor eye drops in challenging cataract surgery. Am J Ophthalmol Case Rep. 2021;25:101245.
- Schoenberg ED, et al. Refractive outcomes of Descemet membrane endothelial keratoplasty triple procedures (combined with cataract surgery). J Cataract Refract Surg. 2015;41:1182–1189.
- Price MO, et al. Implantation of presbyopia-correcting intraocular lenses staged after Descemet membrane endothelial keratoplasty in patients with Fuchs dystrophy. Cornea. 2020;39:732–735.
- Price DA, et al. Initial results of DMEK combined with cataract surgery and implantation of the light-adjustable lens. J Cataract Refract Surg. 2024;50:270–275.
Relevant disclosures
Price: RxSight
Syed: None
Contact
Price: fprice@pricevisiongroup.net
Syed: zsyed@willseye.org