Refractive: YES Connect
Summer 2024
by Ellen Stodola
Editorial Co-Director
We are living in an age where we can deliver some of the most precise refractive results to patients to help meet their expectations and lifestyle needs. Yet the one thing we cannot do is predict with absolute certainty which patients will not be completely satisfied with their results or adapt flawlessly to new lens technologies. As a cataract surgeon, it is important to be comfortable managing patients in these situations. In this issue’s YES Connect column, we explore the ins and outs of IOL exchange. The initial steps a surgeon takes in diagnosis and communication can set them up for success. Allison Chen, MD, and Yvonne Wang, MD, are both cornea and refractive specialists who perform IOL exchanges for a multitude of reasons. Here they discuss some vital tips for every cataract surgeon to be familiar with. IOL exchanges can be a very rewarding experience, both for the surgeon and the patient. I’m excited to share the expert advice of these two phenomenal surgeons with the YES community as we strive to meet the needs of our patients.
—Masih Ahmed, MD, YES Connect Editor
When it comes to doing an IOL exchange, there are a variety of factors involved in why the patient may be unhappy and how to proceed. Yvonne Wang, MD, and Allison Chen, MD, discussed scenarios where an IOL exchange may be necessary and techniques to perform it.
Common scenarios
Dr. Chen said that the most common reasons patients are referred to her for an IOL exchange are poor quality vision with multifocal or EDOF IOLs, UGH syndrome, persistent positive or negative dysphotopsias, or unexpected refractive outcomes. Positive dysphotopsias usually occur due to diffractive optics, and poor quality of vision can occur with diffractive optics or non-diffractive EDOF IOLs.
Dr. Wang said she is also most commonly referred patients for IOL exchanges when the patient is unhappy with a multifocal lens due to the dysphotopsias. They end up seeing much more glare or it’s not the quality of vision they want, so you could exchange that lens for a monofocal lens. She has also encountered a few scenarios where it was necessary to exchange a monofocal to a different type of monofocal because of dysphotopsias. This typically requires switching to one with a lower index of refraction. “It is important to discuss the risk of glare and halos when consenting patients for multifocal IOLs,” she said.
Another scenario, according to Dr. Wang, is when a patient is unhappy with their refractive outcome. This could mean that they ended up more hyperopic or myopic than expected or they wanted to be corrected for distance vision with a monofocal lens but are then unhappy with the loss of near vision. “In these scenarios, I would first offer non-surgical options such as glasses or contact lens correction. If they do not accept that, laser correction would be the next step. However, not all patients are candidates for laser correction or some strongly prefer a lens exchange.”
Dr. Chen added, “If a patient is very motivated for a trifocal IOL to decrease spectacle dependence, I’ll often first put it in the non-dominant eye to see if they are able to tolerate the potential glare. If they are happy with it, we can do the same for the dominant eye, but if they want less glare in the dominant eye, we can place a monofocal.”
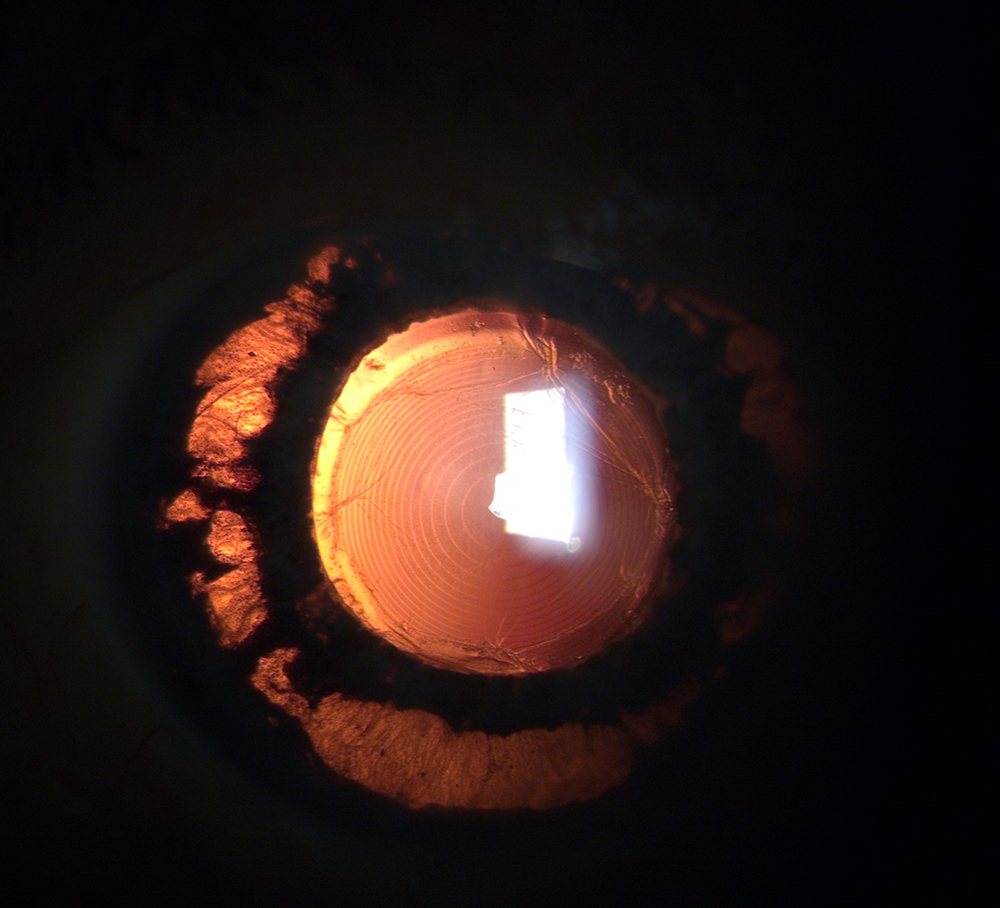
Source: Allison Chen, MD
When to exchange
Dr. Wang said this may depend on if you’re the primary surgeon or if the patient was referred to you. If you are the primary surgeon or had the patient referred soon after the initial surgery, Dr. Wang said she may be more likely to offer an exchange on the early side.
If the problem is a large refractive surprise, you want to exchange sooner rather than later, she said, but if it’s dysphotopsia, she will encourage them to wait at least 3 months. But you have to judge patients individually. If the patient has complaints immediately after surgery, she’s careful not to do YAG capsulotomy, keeping in mind that exchange is a possibility.
In cases of UGH syndrome, Dr. Chen will exchange the IOL as quickly as possible to decrease further intraocular inflammation. For vision quality issues and dysphotopsias, she monitors for at least 3–6 months to assess for symptom improvement prior to exchanging. “I also carefully evaluate the ocular surface to ensure that it is optimized,” she said. “In cases of refractive surprises, I monitor at least 3 months to ensure stability of refraction given it takes time for the IOL to settle into its final effective lens position in the capsular bag.”
Dr. Chen also describes to the patient the potential reasons as to why they may be having visual symptoms and addresses other possible etiologies such as surface dryness or irregularities. “Once all else is optimized, we can proceed with IOL exchange if the IOL itself is the most likely reason for vision problems,” she said. “I also emphasize that sometimes certain ‘brains,’ rather than the person, do not ‘like’ certain IOLs.”
Techniques
The technique used for IOL exchange depends on the lens that was placed, Dr. Wang said. It’s important to know what lens is in the eye.
Dr. Chen said, “In cases of refractive surprises, if I know the initial IOL that was placed, this helps me more accurately calculate the power of the IOL that it should be exchanged for. In these situations, sticking with the same type of IOL can increase accuracy of the refractive outcome.”
Another possible scenario is when a lens has come loose. That is technically an exchange as well. You could have a lens that was placed 10–15 years ago and it becomes loose or dislocated for a variety of reasons.
If there is a stable capsular bag, the best outcome is to exchange from within the bag to within the bag. As long as they do not have an open capsule, we can do bag to bag, Dr. Wang said. If they have a very small opening in the capsule, you can attempt to do bag to bag, but it may be more difficult because often the capsule opening enlarges a bit during surgery, Dr. Wang said. In such cases, the implanted lens can be placed in the sulcus. However, there are more limitations as to which type of IOLs can be safely placed in the sulcus, so it is important to have the right lens available. “Even if I plan to exchange a lens bag-to-bag, I have a sulcus lens available as a backup in case the bag becomes compromised,” she said.
If the lens is loose, there is no capsular support, and you need to exchange it out, she said, this can involve taking out the entire lens-bag complex and placing a secondarily fixated IOL (scleral fixated with or without sutures).
Depending on the patient and the stability of their capsular anatomy, Dr. Chen will perform either in-the-bag IOL exchanges or explantation and removal of the IOL and capsule (if compromised) with secondary IOL implantation via either flanged intrascleral haptic fixation (ISHF) or scleral-sutured IOL techniques. If there is a 3-piece lens already in the eye that needs to be repositioned or scleral fixated due to dislocation or UGH syndrome, she will usually first consider re-scleral fixating the same IOL to minimize trauma to the corneal endothelium.
Tips and tricks
Dr. Wang recommended starting off with having a good discussion on expectations and patient goals and taking your time. It’s also important to have a surgical plan and share this with the patient.
Knowing what type of lens is in the eye is key, Dr. Wang said, especially if it’s been a bit of time. The way the lens get fibrosed into the capsule depends on the shape of the lens.
It’s also important to know how you want to get the lens out of the eye. There are many ways to do this. You can fold and pull it out, cut it completely and pull it out in halves and thirds, or cut it in half, fold, and pull out. You need to make sure you have the right instruments to do it, Dr. Wang said, adding that certain lens materials can’t be cut, so it’s important to know if this is the lens you’re dealing with.
Dr. Chen also mentioned the differences among types of IOLs. Different IOLs tend to fibrose and adhere to the capsular bag in different places, she said. “With enVista lenses [Bausch + Lomb], the adhesions usually occur in the triangular eyelet at the optic haptic junction. With Tecnis single-piece lenses [Johnson & Johnson Vision], the adhesions are most prominent in the cutout indented area at the optic haptic junction, and with Alcon lenses, the capsular fibrosis tends to occur at the terminal bulbs of the haptics,” she said. “When explanting these IOLs, I use a cohesive OVD on a cannula to ensure full release of the adhesions in these areas and sometimes gently lift the capsule while injecting OVD to break the adhesions and to fully open the capsular bag.
“Occasionally, haptics are so fibrosed to the bag that they can’t be released without compromising the zonules. In these cases, to preserve zonular support, I will still open the bag up as much as I can but will amputate the haptics while the IOL is in the bag so that the optic is easier to remove,” Dr. Chen said.
Dr. Chen said in cases where she preserves and re-scleral fixates the existing 3-piece IOL in the eye, she externalizes the trailing haptic and tests the threading of the trailing haptic into a 30-gauge wide lumen TSK needle prior to tunneling the needle for ISHF to ensure that the intraocular threading will proceed smoothly.
“As a precaution, if planning a possible scleral fixation, I obtain permission from the patient’s primary care provider or cardiologist to stop aspirin and blood thinners prior to surgery if safe for the patient,” she added.
About the physicians
Allison Chen, MD
Assistant Professor
Cornea, Anterior Segment, and Refractive Surgery
Department of Ophthalmology
Baylor College of Medicine
Houston, Texas
Yvonne Wang, MD
Assistant Professor
Department of Ophthalmology and Visual Science
Yale School of Medicine
New Haven, Connecticut
Relevant disclosures
Chen: None
Wang: None
Contact
Chen: Allison.Chen@bcm.edu
Wang: yvonne.wang.yw752@yale.edu