Glaucoma
Summer 2024
by Ellen Stodola
Editorial Co-Director
During the 2024 ASCRS Annual Meeting, a symposium moderated by Manjool Shah, MD, and Nathan Radcliffe, MD, featured quick-hit tips from glaucoma specialists. Panelists were asked to share a 1-minute pearl in a variety of categories and included Sarah Van Tassel, MD, Kuldev Singh, MD, MPH, Douglas Rhee, MD, Lorraine Provencher, MD, and Christopher Teng, MD, MBA.
Maximizing your diagnostics
Dr. Van Tassel’s diagnostic pearl was to think of the ganglion cell layer as the “how worried should I be” index. She said to get ganglion cell layer for every patient.
Dr. Singh’s pearl was to only perform tests that will likely impact therapeutic decisions. For example, he said that he generally does not perform OCT testing in patients with advanced visual field loss. OCT is helpful in early disease but not so much in severe disease. Let the course of the disease or where the patient is on the disease spectrum guide what they need in terms of diagnostics, he said.
Dr. Rhee said RNFL measurements are great when they’re normal, but don’t just quickly glance at them without looking at the year-to-year transition. Don’t forget green disease, he said, where you can have progression. If the line moves and shifts down, even if it’s still in the green zone, this can be progression.
Dr. Provencher encouraged everyone to get in the VR visual field groove. It can improve your workflow, it’s portable, and it’s loved by technicians and patients, she said. Oftentimes, you’ll get a more reliable visual field result due to improved patient comfort. There are several products available so when choosing a product, do your research. The product should have a strong correlation with HVF, proper background luminance, and validation for all ranges of severity.
Dr. Teng’s diagnostic pearl was that OCT macula is key. You can’t diagnose what you can’t see, he said.
Source: Christopher Teng, MD
Laser tips
Dr. Van Tassel encouraged everyone to confirm (and reconfirm) laser settings. With the dual mode capsulotomy/SLT laser systems, it’s possible to inadvertently use SLT laser beam to perform capsulotomy. The literature tells us that it happens, she said, and it’s associated with vision loss.
Dr. Singh’s laser pearl was to do less more often rather than doing more less often. The future of laser is doing regular treatments, he said, and he expects that ongoing research will support this approach. In the past, we have done SLT and waited for the effect of the treatment to be lost before treating again. The concept of maintenance SLT at regular intervals, to avoid periods of time when IOP is not well controlled, is gaining traction.
Dr. Rhee’s laser tip referenced the Laser in Glaucoma and Ocular Hypertension (LiGHT) trial. The data has been out since 2022 that patients who start with laser do better with IOP control, visual field, and fewer numbers of interventional glaucoma surgery.
Dr. Provencher’s tip pertained to the XEN Gel Stent (AbbVie). “When in doubt, YAG it,” she said. If you see sudden, late XEN failure, do gonioscopy first. If the XEN looks grossly normal, consider occult intraluminal cellular debris. Before you needle the bleb, perform YAG laser just anterior to the internal ostium of the XEN to create a fluid “shock wave” to clear the lumen. Success is when you see the pressure drop and the bleb rise.
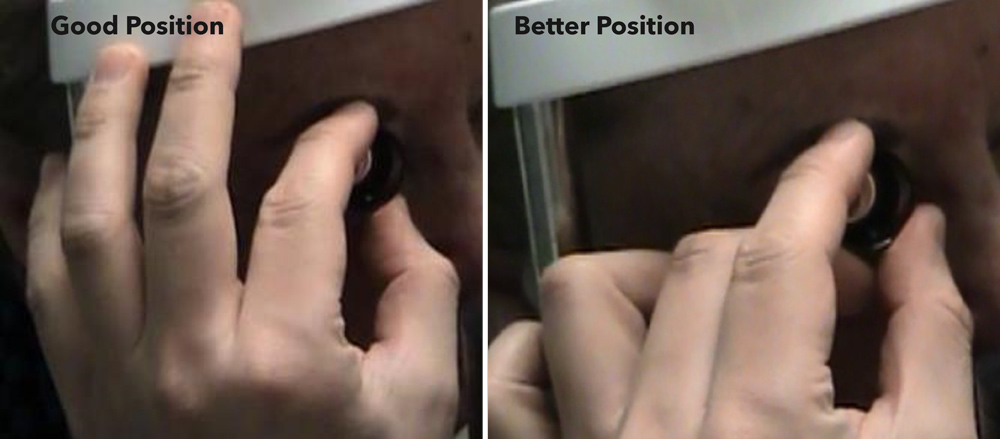
Dr. Teng said that hand positioning is important. In order to achieve a smooth 360 rotation with the Abraham lens, hold the lens with the thumb and index finger, and place the middle finger under the lens, he said. The middle finger supports the lens, thereby enabling the rotation.
Medications/sustained delivery
Dr. Van Tassel said don’t wait for patients to complain about side effects. There are a lot of reasons that patients will withhold a complaint. They may be uncertain of the connection between the drop and the effect, there may not be time during their visits, or they may not have the confidence. But she said not to wait. Most glaucoma is asymptomatic, and the treatment shouldn’t be worse than the disease.
Dr. Singh’s pearl was when possible, make no more than one change at a time when adjusting therapy. Since IOP fluctuates over time, and the IOP-lowering effects of a particular treatment vary among patients, assessing the impact of a single treatment change is difficult enough. Making multiple changes at one time makes assessment even more challenging.
Dr. Rhee said that sustained release bimatoprost (also even topical PGAs) have a prolonged effect in some patients. He added that bimatoprost induces lymphangiogenesis-like changes. Efficacy of bimatoprost sustained release is no worse than goniotomy done without cataract surgery.
Dr. Provencher reviewed the flaws of topical medications, like ocular surface disease, compliance issues, etc. “Our dream would be to have 100% intervention, 100% control, and 0% topicals. However, the reality is meds do still play a role as bridge therapy or because of poor access to a surgeon or patient preference.” When one must use meds, Dr. Provencher encouraged surgeons to choose wisely, selecting options with a novel mechanism of action that keeps conventional outflow open, like ROCK inhibitors. Reach for meds that work synergistically with interventional glaucoma.
Dr. Teng suggested using the jab technique. The cornea has many layers, he said. If you use a constant force, when you break through the cornea, you will advance far into the AC and may hit the iris, lens, or deeper. By jabbing, you naturally stop yourself before going too deep. It takes 2–8 jabs to break through, and this comes in handy on soft or firm eyes, Dr. Teng said.
MIGS
Dr. Van Tassel said to use MIGS as an opportunity to reset. She said to work hard to reduce or eliminate drops. It’s also a great time to deploy SLT or sustained release, if the patient is not at his or her goal. If needing to add back drops, optimize simplicity, tolerability, cost, and efficacy.
Dr. Singh’s pearl was to choose procedures based on safety and efficacy, not reimbursement. He pointed out that over the past few years, large shifts in which glaucoma procedures are performed have been seen following reimbursement changes. Such changes suggest that reimbursement, rather than efficacy and safety data, has been the primary driver of what procedures patients receive. Hopefully, this will not be the case in the future, he said.
Dr. Rhee said not all MIGS devices are the same. Evidence from the COMPARE clinical trial showed that the Hydrus Microstent (Alcon) has better IOP control. Furthermore, two separate laboratory studies using cadaver eyes found better enhancement of outflow with the Hydrus.
Dr. Provencher’s pearl related to avoiding hyphemas. Intraoperatively, use reverse Trendelenburg, leave the final IOP in the mid-20s, and if you get hyphema coming from the angle, leave a strip of dispersive OVD in that area. In the first 24 hours, Dr. Provencher is strict with activity precautions, and she added that cataract plus MIGS is not the same as cataract surgery. She asks patients to sleep with the head of the bed elevated 30–45 degrees for the first night. She also has strict postop lifting precautions and institutes shield use to prevent rubbing.
Dr. Provencher offered an additional tip, a mnemonic (M-STAGES) she created to help providers decide when to “go big” (like an incisional surgery) or when to stick with MIGS.
- M – Mechanism of disease
- S – Severity
- T – Target IOP
- A – Age
- G – Gtt tolerance and duration of use
- E – Expectations of the patient
- S – Synergy with cataract surgery
Dr. Teng’s MIGS pearl was to use the wound as a fulcrum. With the device in the eye, tilt forward on the wound to pivot the eye in order to maximize the view.
Source: Lorraine Provencher, MD
Incisional glaucoma
Dr. Van Tassel said for gel stents, look for luminal flow. Be meticulous and patient about anterior chamber irrigation until luminal flow is observed, she said. What’s important is that you lift the Tenon’s over the tissue, and be sure there is no Tenon’s entanglement with closure. Her bonus pearl was that she has found better refractive outcomes with the modified Wise/Condon closure.
Dr. Singh’s pearl was that trabeculectomy beats all other procedures in patients with advanced disease who are at substantial risk of blindness from glaucoma. In addition to lowering IOP better than any other procedure, trabeculectomy is more likely to get patients off of IOP-lowering medications. Having a low IOP without medications decreases the likelihood of IOP swings related to non-compliance as well as peak and trough effects of such drugs. Better IOP control without medications is more likely to preserve vision.
Dr. Rhee said trabeculectomy with anti-metabolite is still the gold standard for incisional glaucoma surgery. More invasive glaucoma surgery is most reliable to achieve less than 12 mm Hg IOP and is most able to be adjusted postoperatively, he said. It’s also the most likely to help patients be medication-free postoperatively.
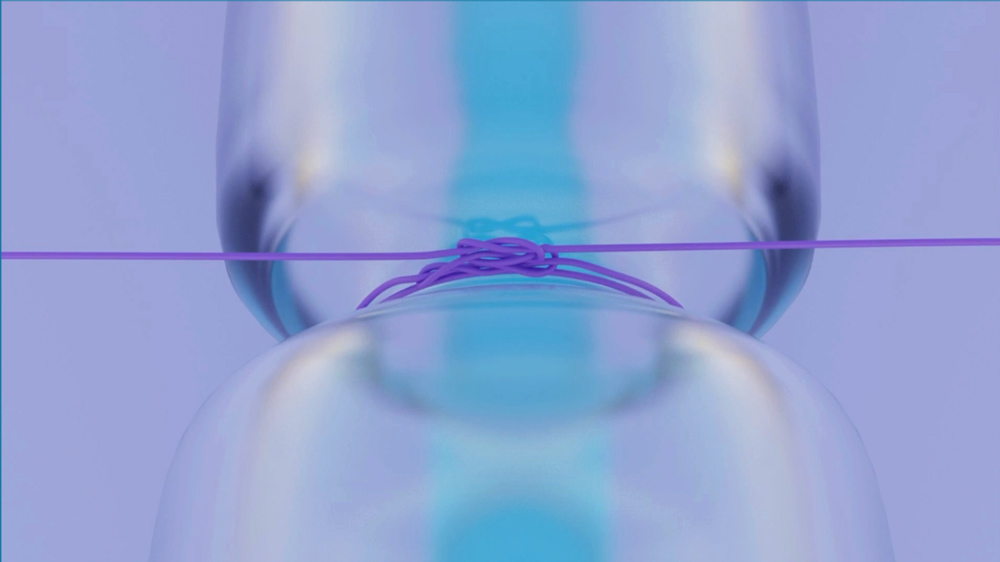
Dr. Provencher discussed her “OctoKnot” non-valved tube occlusion technique for how to occlude a non-valved tube to get a watertight closure.
Dr. Teng said that a stepwise approach to incisional glaucoma surgery is OK. He listed several steps.
- Step 1: TM bypass stent, goniotomy, viscocanalostomy
- Step 2: Ab interno trabeculotomy +/–viscocanalostomy
- Step 3: Microinvasive bleb-forming surgery
- Step 4: Trabeculectomy or glaucoma drainage implant
Article Sidebar
Access ASCRS On Demand
ASCRS physician registrants to the ASCRS Annual Meeting have on demand access to this and other sessions from the meeting.
About the physicians
Lorraine Provencher, MD
Vance Thompson Vision
Omaha, Nebraska
Douglas Rhee, MD
Professor and Chair
University Hospitals
Case Western Reserve University School of Medicine
Cleveland, Ohio
Kuldev Singh, MD, MPH
Professor of Ophthalmology
Chief of the Glaucoma Division
Stanford University School of Medicine
Stanford, California
Christopher Teng, MD, MBA
Associate Professor of Ophthalmology and Visual Science
Yale University School of Medicine
New Haven, Connecticut
Sarah Van Tassel, MD
Associate Professor of Ophthalmology
Weill Cornell Medicine
New York, New York
Relevant disclosures
Provencher: Alcon, Allergan, Beyeonics, Elios Vision, Glaukos, MicroSurgical Technology, New World Medical, Thea, Vialase
Rhee: AbbVie, Alcon, Iantrek
Singh: Alcon, Belkin Vision, Elios Vision, Novartis, Santen, Sight Sciences
Teng: None
Van Tassel: AbbVie, Allergan, Carl Zeiss Meditec
Contact
Provencher: lorrainemprovencher@gmail.com
Rhee: dougrhee@aol.com
Singh: kuldev@yahoo.com
Teng: christopher.teng@yale.edu
Van Tassel: sjh2006@med.cornell.edu


