Glaucoma
April 2023
by Ellen Stodola
Editorial Co-Director
MIGS procedures have become a mainstay in the surgical treatment of mild to moderate glaucoma, but what pressures can physicians realistically expect with these? Several physicians discussed this, as well as how MIGS can fit into the overall glaucoma management process and what to do if MIGS procedures don’t achieve the desired IOP.

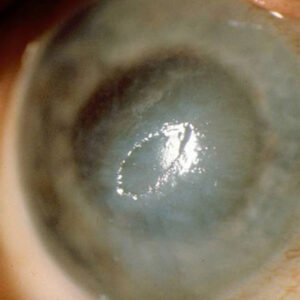
Source: Arsham Sheybani, MD
Before getting into the discussion about IOP levels attainable with MIGS, Arsham Sheybani, MD, stressed the importance of case selection from the beginning. “You’re trying to avoid having the MIGS fail, and in general, patients who have been on medications for years or who have more advanced disease aren’t going to do well with angle procedures,” he said.
“[With] MIGS in general, if you need pressures that are consistently going to be in the low-teens without medications, angle surgery is not going to be a great option,” Dr. Sheybani said. “On average, the way to avoid failure is to do [MIGS] in patients where your goal pressures are in the mid-teens, and they have some tolerability to at least one class of medications.”
If you are operating on a patient’s cataract and that’s the main reason for surgery, Dr. Sheybani said it may be reasonable to try an angle surgery, but for advanced disease, if the pressure is high, there’s unlikely to be a significant reduction with angle surgery.
Kuldev Singh, MD, said the IOP levels that can be expected after angle-based MIGS surgery are usually similar to preoperative IOP but with reduced dependence on medications.
“I think that’s the most achievable goal of MIGS—to reduce the number of medications,” Dr. Singh said, adding that there will be some patients who can get lower pressures if they were not on medications previously, but the main goal is to get patients off as many medications as possible. Dr. Singh thinks there will be data forthcoming that will show that if you achieve the same IOPs with or without IOP-lowering medications in similarly diseased patients, eyes that are off medications will do better in terms of visual field preservation than those where medications continue to be needed.
Dr. Singh said he mostly performs traditional glaucoma procedures, like trabeculectomy and tube implants. These, he said, “are the ones that can sometimes prevent patients from going blind from glaucoma.” He sees MIGS as an option for patients with mild to moderate disease or controlled glaucoma and a need for cataract surgery. “But for patients who have a substantial risk of blindness from glaucoma, MIGS are much less likely to get you to the pressure goal, and you often need to accept the risks that come with trabeculectomy to have a reasonable chance of preserving vision,” Dr. Singh said. “I think the greatest value of canal-based MIGS is that each eye undergoes cataract surgery only once, presenting an opportunity to adjunctively do something good for the glaucoma. … You can piggyback onto cataract surgery, which alone results in IOP lowering, and get an additional benefit from the MIGS procedure.”
With a variety of MIGS devices and procedures available, Dr. Sheybani said the choice depends on the disease.
First, he mentioned partial goniotomies, which he expects would be done at the time of cataract surgery and can get pressure to 14–15 mm Hg. Dr. Sheybani added that you should be able to get patients off one or two classes of medications with this. “If they started at two to three, they might be down to a drop at 1 year,” he said.
If using partial goniotomy as a standalone procedure, Dr. Sheybani said it’s unlikely to show a large pressure drop. When he performs goniotomy as a standalone, he said it’s usually 180–360 degrees. “We have the iTrack catheter [Nova Eye Medical], OMNI Surgical System [Sight Sciences], sutured GATT, and they can get pressure down as a standalone procedure.” However, there is a risk of bleeding. Secondary open-angle glaucoma patients do much better in those cases, he explained. “We’ve had uveitics with pressures in the 40s who you can get down into the teens and off their drops, if you get to them early enough,” he said.
Dr. Sheybani said if he’s already worked in the angle, he will not go back in if the patient isn’t where they need to be. He will engage a subconjunctival option if he’s already tried an angle procedure, like stenting or goniotomy.
That’s where the conversation gets a little more nuanced, he said. With a stent, like Hydrus (Alcon), you have the ability to access at least a few collector channels with the way it is placed. Compared to the first-generation iStent (Glaukos), Hydrus has a better pressure reduction and less need for secondary surgical intervention, he said.
Dr. Sheybani also said he will not go back in the angle if he’s already been there because he wants to do as much as he can at the time of the procedure in the angle. “If I’m doing an iStent or a Hydrus, I’m trying to pick the cases where it’s going to get the maximum efficacy with that device,” he said. “We’re not going to try to push it in someone with advanced disease or someone with high pressure looking to get a dramatic pressure reduction.”
Sameh Mosaed, MD, has been performing MIGS since 2003. “The IOP levels you can expect with someone on medications in whom you do MIGS in combo with phaco or even standalone is in the mid-teens, and if you supplement it with medications, you can get it to the low teens,” she said.
When performing MIGS in combination with cataract surgery, Dr. Mosaed thinks it’s a good trade-off to have moderate IOP lowering with less medications. But she noted that she won’t typically perform MIGS as a standalone procedure just to reduce the medication burden. “The place where it fits into my practice as a standalone procedure is in the setting of steroid-induced glaucoma where the patient will come in with a very high pressure in the 30s–40s, sometimes 50s; the trabecular bypass procedures work well for steroid-induced glaucoma,” she said.
When Dr. Singh chooses a MIGS procedure, he looks for options where there is high quality data to support the use. He noted that many of the implantable MIGS devices went through rigorous review processes for approval, so there is a lot of data on safety and efficacy. “Some of the most robust trials done by the glaucoma community were for implantable MIGS procedures,” Dr. Singh said. He thinks that the quality of long-term efficacy and safety data available for adult goniotomy is insufficient presently, thus he has not incorporated this procedure in his practice. Dr. Singh also said that reimbursement plays no role in his decision making, and he has been disappointed by trends suggesting that the use of various MIGS devices in the U.S. has been influenced by levels of and changes in reimbursement.
Determining if a MIGS procedure worked or if it’s necessary to try a different approach depends on a couple of factors, Dr. Sheybani said. First is the severity of the patient’s glaucoma. “I tell patients that we might not know where the pressure will settle until a couple months after the procedure because then I’ve been able to taper steroids,” he said, explaining that you need 4–6 weeks to know the steroid effect is washed out.
The earliest Dr. Sheybani said he would go back in would be around 2 months after a procedure, though it’s uncommon. These would be cases where the patient’s collectors weren’t going to work no matter what, or perhaps the stent isn’t in the right spot.
“If you’re taking a patient in [and doing a MIGS procedure] for drop irritability or compliance issues, you should make sure your procedure can reduce medication load,” Dr. Sheybani said. “I always tell patients that it’s a marriage between the medicines and the surgery.” Sometimes the surgeries can’t lower the pressure to what it needs to be, and medicines will get these patients the rest of the way, he said.
Dr. Mosaed said that she finds that patients are often still enjoying a pressure reduction years later. “I think patients fall into two broad categories: those in whom it’s very minimally effective and doesn’t do much for them, and those in whom they get a nice robust pressure response, and in those, it does tend to be sustained for many years,” she said.
Even though you’re bypassing the trabecular meshwork where you would expect any steroid effect to be playing a role, Dr. Mosaed said there’s still a lot of fluctuation in pressure during the early postop period when patients are using steroids and physicians are titrating their glaucoma medications and trying to figure out where they land. “I will give them at least a couple of months to figure out if we need something more,” she said, adding that in the rare case that the patient has a sustained IOP spike, she will take them to surgery quickly.
When discussing combination MIGS, Dr. Sheybani said two MIGS you often hear being used in combination are the Hydrus and OMNI Surgical System. He said he doesn’t usually combine devices though. One reason for this is that he trains fellows, and he needs them to understand what each device does individually.
Dr. Mosaed said that she has seen many people use MIGS devices in combination, but she does not. “If you’re attempting to do moderately effective procedures in combination to try to get the pressure down dramatically, these all add cost and additional unknowns on top of one another,” she said. “Most of the MIGS do function through similar methods, like bypassing the trabecular meshwork. If you’re doing MIGS that function through different mechanisms of action, combining those might be a better approach.”
In general, though, Dr. Mosaed said, doing combination MIGS might not make sense “when you do have trabeculectomy that is cheap and effective and when done by the right hands can give excellent results. “Having had so much experience with a wide range of MIGS and long-term results, I’m a believer and it has a place in my armamentarium. However, I still have a deep respect for trabeculectomy and tube shunts,” she said. “I think knowing how to do a good trabeculectomy is very much a value, and I don’t want MIGS to appear so technically less demanding as to make people lose interest in maintaining trabeculectomy skills.”
This is key in the training of residents and fellows, Dr. Mosaed said. It’s critical to provide solid trabeculectomy training because it’s the single most effective IOP-lowering procedure to date. “Many of these training programs are teaching more MIGS, less valveless tubes and even less trabs,” she said. “Coming from a place where I’ve done all of them for 20 years, I can say that they all have their place, but nothing beats a trab.”
Discussing trabeculectomy, Dr. Sheybani described it as a “powerful surgery,” but he said the consequences can be powerful, too. With MIGS, the risk for vision loss related to surgery is lower, but these devices don’t lower the pressure as much.
Much depends on the timeframe and how early you’re able to treat the patient. “If we operate earlier and can predict who’s going to get into trouble sooner, I think these MIGS procedures have even more value,” he said.
Dr. Singh noted the importance of continuing to train surgeons on traditional glaucoma procedures even as the MIGS field advances. “I foresee a public health problem in the future if there aren’t enough people trained in trabeculectomy to prevent those who need it from going blind from glaucoma,” he said. The field is moving in parallel, he said, with some trying to make traditional surgery better and others trying to refine MIGS to better care for those with mild disease. “To me, those aren’t mutually exclusive. You can do both,” he said. He also thinks that practitioners who did not receive the necessary training to make trabeculectomy as safe and effective as possible in their practices may gravitate to other bleb-forming options. But he agreed with Dr. Mosaed that nothing beats a trabeculectomy when done by the right hands.
About the physicians
Sameh Mosaed, MD
Director of the Glaucoma Service
Gavin Herbert Eye Institute
University of California Irvine
Irvine, California
Arsham Sheybani, MD
Associate Professor, Ophthalmology and Visual Sciences
Washington University School of Medicine in St. Louis
St. Louis, Missouri
Kuldev Singh, MD
Professor and Chief of the Glaucoma Division
Stanford University School of Medicine
Palo Alto, California
Relevant disclosures
Mosaed: Alcon, Sight Sciences
Sheybani: AbbVie, Alcon, New World Medical, Nova Eye Medical, Santen, Sight Sciences
Singh: Alcon, Allergan, Glaukos, Santen, Sight Sciences
Contact
Mosaed: smosaed@hs.uci.edu
Sheybani: arsham.sheybani@gmail.com
Singh: kuldev@yahoo.com