Cataract
June 2022
by Liz Hillman
Editorial Co-Director
The application of anterior segment OCT (AS-OCT) in cataract surgery is relatively new.1 The authors of a 2021 review of AS-OCT described the current role of the technology and perspectives and its potential future application, concluding:
ASOCT technology is comprehensively making progress in the assessment of cataractous eyes in the preoperative as well as intraoperative periods. The positive role of ASOCT in objectifying the cataractous grade, intralenticular changes in white/mature cataracts, and posterior capsular changes in posterior polar and traumatic cataracts cases demonstrates its definite adjuvant role in routine clinical practice. In addition, compared to previous technologies, emerging swept source technology has furthered the cross-sectional imaging as a more practical tool. Hence, ASOCT is likely to become an integral part of assessment when dealing with complex lenticular entities in future.
The authors of a chapter in the book OCT Applications in Ophthalmology described the various ways in which they saw value of the technology for cataract surgery, including “(1) anterior lens capsule and lens epithelium evaluation using spectral-domain OCT (SD-OCT); (2) investigation of clear corneal incision in femtosecond laser assisted cataract surgery using SD-OCT; (3) capsular block syndrome evaluation before and after treatment using SD-OCT; and IOL power calculation in post-myopic excimer laser eyes using SD-OCT.”2
A book chapter in High Resolution Imaging in Microscopy and Ophthalmology: New Frontiers in Biomedical Optics described the various technologies with anterior segment OCT capabilities.3 While many applications are related to cornea (which can have implications on refractive cataract surgery), some technologies have increasing applications that can aid in IOL calculations, the authors wrote.
Preop and postop applications
Kevin M. Miller, MD, said preoperative and postoperative imaging with AS-OCT can be helpful.
“Preoperatively, anterior segment OCT can be used to identify posterior capsule openings or posterior lenticonus in eyes with posterior polar cataracts,” he said. “It can also be used to define the shallowness of an anterior chamber or document the presence of iridocorneal adhesions.”
Dr. Miller said that he’s selective as to when he’ll use AS-OCT preoperatively. He’ll only use it preop if a posterior polar cataract is present. Intraoperatively, he’ll use it as part of the process of performing FLACS.
Postop, Dr. Miller listed five possible applications for AS-OCT:
- Look for/document the presence of retained lens fragments in the anterior chamber
- Identify Descemet’s membrane detachments in eyes with edematous corneas
- Document the presence of capsular block
- Look for epithelial or fibrous ingrowth
- Look for IOL tilt and/or decentration
He added that he finds identifying Descemet’s membrane detachments to be especially helpful when he can’t figure out why it is taking so long for an eye to recover from surgery.
Abhay Vasavada, MD, said he relies on anterior segment OCT frequently, finding it useful in cases of chronic angle closure glaucoma, pseudoexfoliation, eyes with zonulopathy, posterior polar cataract, and pediatric cataract (if the child can sit for it).
“I think the modern technology of the anterior segment OCT is helping in different scenarios where cataract surgery is done. With a shallow anterior chamber, for example, in many of these there are loose zonules, which can lead to the forward movement of the zonular-capsular bag. If you can see on anterior segment OCT, you are prepared for your strategy because sometimes, even if you do in-the-bag IOL implantation, because the zonules are weak or loose, the IOL remains forward, and sometimes that shallowing of the chamber can lead to so-called angle glaucoma,” Dr. Vasavada said.
In eyes with known chronic angle closure glaucoma, he said anterior segment OCT can show and validate the change—space created and ciliary body rotation—from preop to postop. “You can see the restoration to some extent of the anterior segment anatomy,” Dr. Vasavada said.
Dr. Vasavada added that he’s used AS-OCT for a long time in cases of posterior polar cataract. For these, it can help determine the location and extent. If it’s unclear on slit lamp exam if it’s a plaque or posterior polar cataract, Dr. Vasavada said AS-OCT can provide that additional assurance.
“I think if you want to deliver the best care … it is useful to incorporate anterior segment OCT,” he said, adding that there is an increasing trend in the use of this technology in the context of cataract surgery.
Intraoperative potential
Ronald Yeoh, MD, shared some of his insights about intraoperative OCT for cataract surgery. He said intraoperative OCT was introduced several years ago as a tool for vitreoretinal surgeons to assist in peeling the epiretinal membrane and internal limiting membranes from the macula, as well as to assist corneal surgeons as they visualize corneal layers during lamellar surgery.
“It was interesting that in the marketing literature provided, there was no mention of its use in cataract surgery, despite the fact that cataract surgery has more volume than retinal and corneal surgeries put together,” Dr. Yeoh said. “This was maybe because there was a perception that modern phaco cataract surgery is so well developed that an added imaging technique like intraoperative OCT would not be useful to cataract surgeons. On the contrary, I have found that intraoperative OCT has opened up a new dimension in phaco cataract surgery.”
First and foremost, Dr. Yeoh said intraoperative OCT is helpful for the teaching of trainees.
“We are operating on a 3-D structure, and intraoperative OCT allows us to see the eye in cross section during surgery,” he said. “This leads to a better understanding and appreciation of the surgical anatomy and fluidic movements during cataract surgery. This in turn is an invaluable aid to trainee cataract surgeons who get far more information compared to just a microscopic view.”
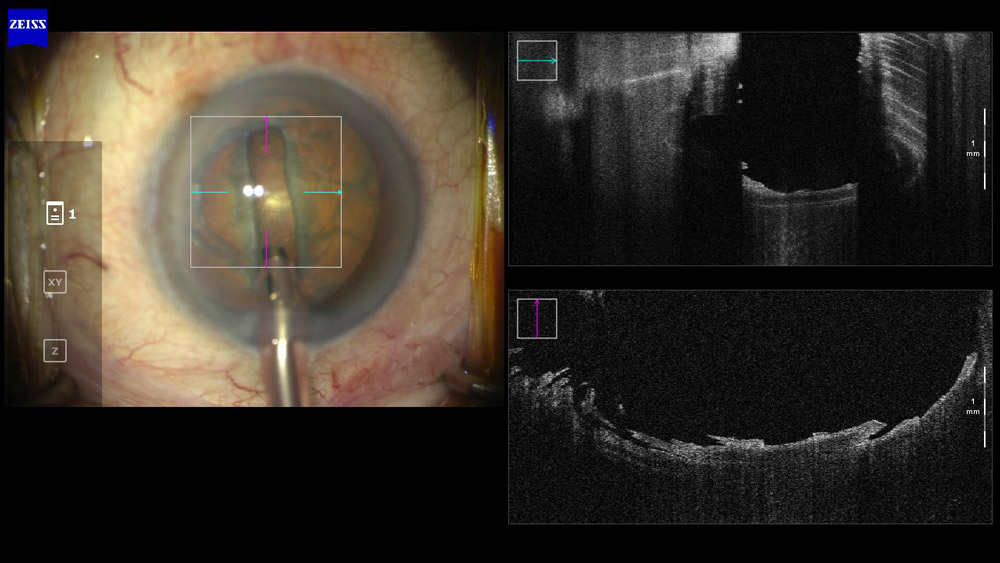

Dr. Yeoh noted how with intraoperative OCT, a trainee can see and adjust his or her technique while sculpting a groove in the nucleus (Figure 1). When inexperienced, knowing how deep to create a groove or how it should be shaped can be difficult.
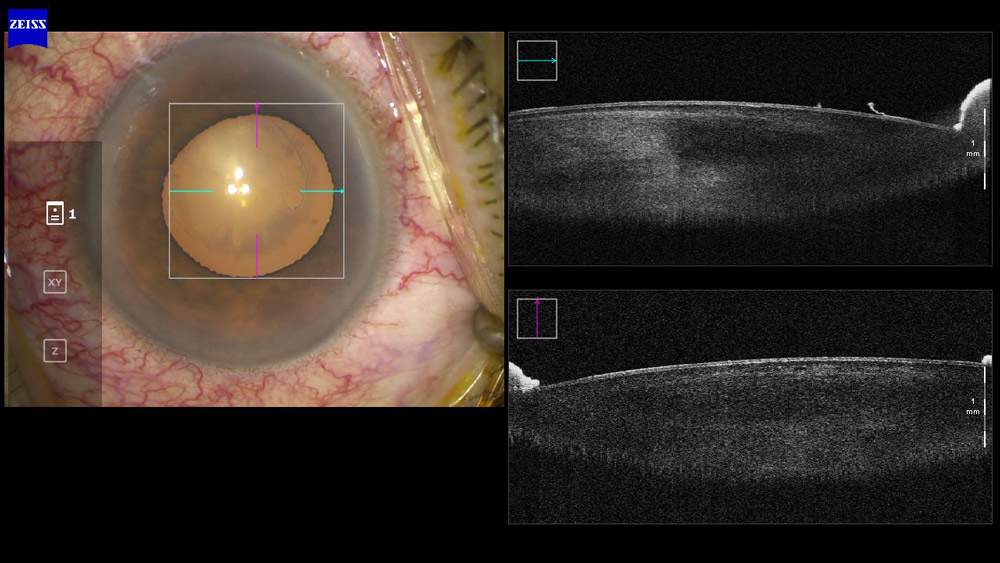
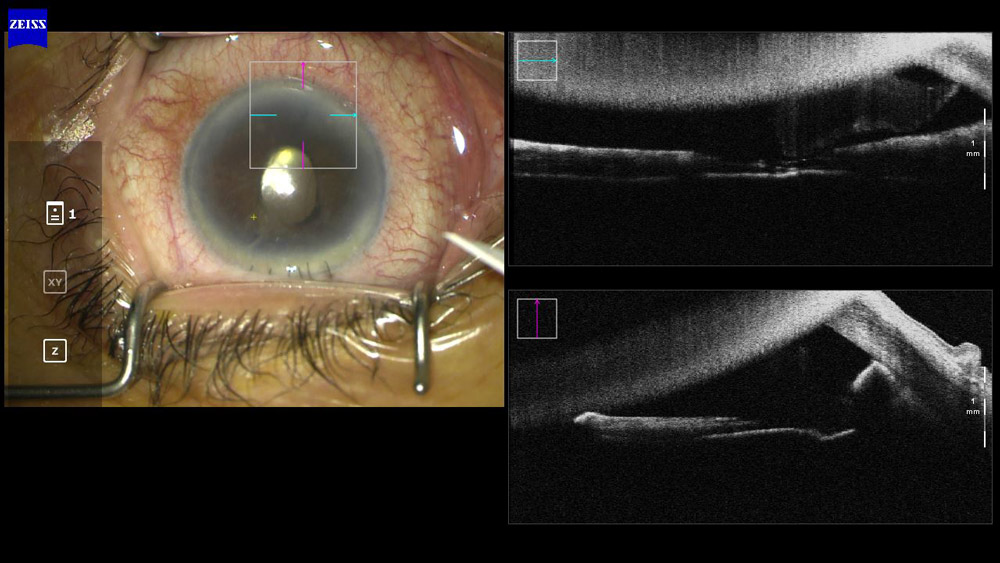
Dr. Yeoh said intraoperative OCT is also helpful in diagnosing a posterior subcapsular cataract vs. a posterior polar cataract (Figure 2) and showing pseudoexfoliation material on the anterior lens surface (Figure 3). He admitted that while this function “gives us pretty pictures, [it] does not always contribute to better or safer surgery.”

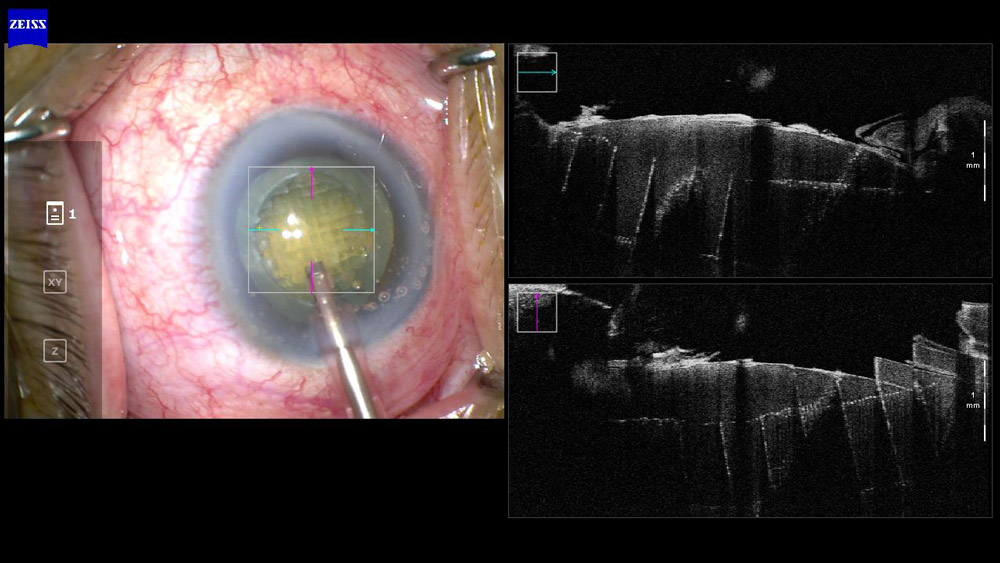
Intraoperative OCT has helped surgeons see and better understand where the fluid planes are in hydrodissection and hydrodelineation. He said that these are brief but important steps in phaco. “In Figure 4, we can see that after hydrodissection, there is a layer of fluid behind the nucleus with a small layer of residual lens cortex still present in front of the posterior capsule. Despite our best efforts to effect cortical cleaving hydrodissection, leaving a clean posterior capsule, this is often difficult to achieve,” he said. “Hydrodelineation, which was also done in this case, results in a golden ring around a small nucleus, and this is reflected by the intraoperative OCT image of a thin line just behind the nucleus.”


Intraoperative OCT can also identify if there is still OVD under the IOL (Figures 5 and 6). As a surgical aid, Dr. Yeoh shared a case where intraoperative OCT was able to detect and show a posterior capsule rupture prior to starting surgery (Figure 7), which allowed the surgeon to modify the technique.
Dr. Yeoh also shared how he was able to image patients with anterior radial tears and posterior capsule ruptures, thanks to intraoperative OCT, when corneal clarity compromised the view or was just difficult to see. “The intact posterior capsule is transparent and difficult to see even with a microscope, and sometimes we are unsure as to whether a posterior capsule rupture has occurred,” he said.
Figure 8 shows a patient who had an anterior radial tear in the capsulorhexis edge and an anterior radial tear extending posteriorly across the whole posterior capsule.


“The anterior radial tear is shown by the two thick, curved lines and the posterior capsule tear by the thinner and more scrolled edges. I named this the ‘intraoperative OCT scroll sign of posterior capsule rupture,’” he said. “They behave differently because we know that the anterior capsule is thicker than the posterior.”
Intraoperative OCT also came to the rescue when a patient was brought back to the OR with a retained nuclear lens fragment. Intraoperative OCT was able to find the fragment in the angle for successful removal (Figure 9).
Dr. Yeoh used imaging from intraoperative OCT to show why less ultrasound energy is needed in FLACS with dense cataracts.
“I prefer to use a laser grid pattern with two horizontal cuts, which effectively softens the nucleus for easy division and removal using less ultrasound energy. In Figure 10, we can see how the grid pattern with horizontal cuts results in little rectangular ‘chips,’ explaining why less ultrasound energy is needed,” he said.
Dr. Yeoh said that while intraoperative OCT was initially considered a “nice to have” feature for cataract surgery, he thinks it’s finding a bigger role in training, surgical decision making, research around wound construction and integrity, IOL positioning, and removal of OVD.
“From an institutional point of view, having cataract surgeons use this technology in cataract surgery makes its acquisition a more economical proposition than just being for corneal or vitreoretinal surgeons’ use,” he said.
About the physicians
Kevin M. Miller, MD
Kolokotrones Chair in Ophthalmology
David Geffen School of Medicine
University of California, Los Angeles
Los Angeles, California
Abhay Vasavada, MD
Director
Raghudeep Eye Clinic
Ahmedabad, India
Ronald Yeoh, MD
Medical Director
Eye & Retina Surgeons
Singapore
References
- Pujari A, Sharma N. The emerging role of anterior segment optical coherence tomography in cataract surgery: current role and future perspectives. Clin Ophthalmol. 2021;15:389–401.
- Wang X, et al. OCT application before and after cataract surgery. OCT Applications in Ophthalmology. 2018.
- Asam JS, et al. Chapter 13: Anterior segment OCT. High Resolution Imaging in Microscopy and Ophthalmology: New Frontiers in Biomedical Optics. 2019.
Relevant disclosures
Miller: None
Vasavada: Alcon
Yeoh: Alcon, Carl Zeiss Meditec, Johnson & Johnson Vision
Contact
Miller: kmiller@ucla.edu
Vasavada: icirc@abhayvasavada.com
Yeoh: ersryeoh@gmail.com

