Refractive
Spring 2026
by Liz Hillman
Editorial Co-Director
Detecting irregular astigmatism is less about classification and more about recognition. As corneal imaging technologies continue to evolve, identifying subtle irregularities early has taken on greater importance—particularly in the context of cataract surgery planning and patient satisfaction. Understanding how these findings are detected, and why they matter clinically, is becoming an essential part of preoperative evaluation and occasionally postop when a patient is complaining of poor visual quality.
Topography has been able to identify irregular astigmatism for decades, and even before that, said William Trattler, MD, manual keratometry, if it didn’t line up properly, was a diagnostic tool.
Source: Stephen D. Klyce, PhD, FARVO, and Marguerite B. McDonald, MD, FACS
Stephen D. Klyce, PhD, FARVO, and Marguerite B. McDonald, MD, FACS, said in an email to EyeWorld that newer, “advanced” corneal imaging technologies can actually be less sensitive in detecting irregular astigmatism compared to Placido- based technologies.
“When evaluating a patient with astigmatism, subtle irregularities are best detected with Placido-based devices, which are 20 times more sensitive than tomography-based devices,” Dr. Klyce and Dr. McDonald said. “Stated differently, anterior corneal maps based on Placido technology are the most reliable and repeatable at detecting early pathology, such as early keratoconus.”
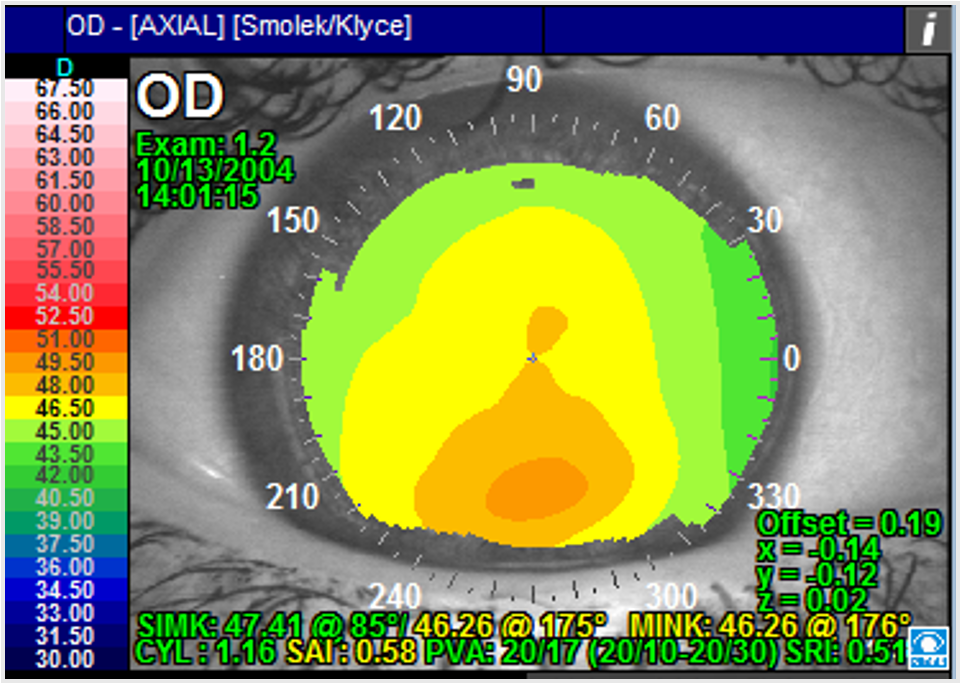
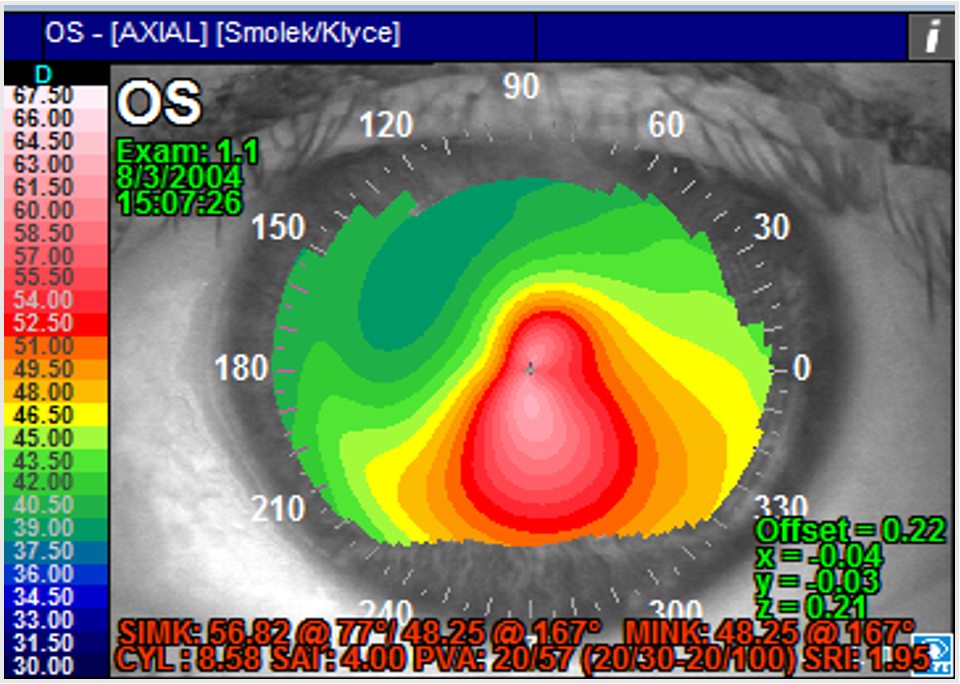
Dr. Klyce and Dr. McDonald provided a short history of the first correlations of corneal irregularities and vision, as demonstrated by corneal topography in 1996, and how it has evolved since. In that early work, irregularities in the mires were reflected in Placido images.
“Small irregularities in the positions of the mires along hemi-meridians were averaged over the central cornea forming an index called the surface regularity index (SRI).1 Correlation with clinical vision data provided the range of potential visual acuity (PVA) that could be attained with a patient’s cornea analyzed with corneal topography (Figure 1),” they said. “After that early work, characterization of irregular astigmatism is typically done by modeling the corneal surface with the Zernike polynomial series of radial basis functions. Zernike polynomials were adopted by the ANSI and ISO Standards groups to describe the components of the distortions produced by irregular astigmatism. These are generally called the higher order aberrations (HOAs), while the lower order aberrations also modeled with the Zernike series are those that are correctable with spherocylindrical optics (including regular astigmatism).”
Dr. Trattler said imaging technologies have become more sophisticated over time, making it easier to identify both regular and irregular astigmatism.
It’s important just to do the imaging, Dr. Trattler said. “There are still many doctors who don’t perform topography prior to cataract surgery, for example. When a screening topography is performed, it’s a non-covered service, so there’s a cost to the practice,” he said. However, missing irregular astigmatism prior to cataract surgery can be a significant source of postop dissatisfaction.
“When we look at patients’ topography prior to cataract surgery, there is a surprising number of patients who have irregular astigmatism, and the topography reveals that,” he said, adding later that treating irregular astigmatism is dependent on what’s causing it.
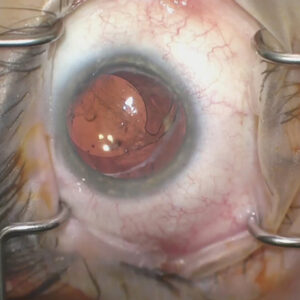
The most common causes of irregular astigmatism are dry eye and epithelial basement membrane dystrophy, but Dr. Trattler mentioned irregularities can also be due to corneal scars, corneal haze, and/or keratoconus.
“Irregular corneal astigmatism not caused by dry eye disease can take many forms and is most often related to trauma, surgical intervention, or pathology,” Dr. Klyce and Dr. McDonald said.
Source: Stephen D. Klyce, PhD, FARVO, and Marguerite B. McDonald, MD, FACS
Another technological newcomer to detecting corneal irregularities is epithelial mapping. Receiving its first FDA approval less than a decade ago, Dr. Trattler said we’ve learned the epithelium isn’t always uniform.
“You can have something called epithelial hyperplasia, where the corneal shape looks like keratoconus, but it’s not. It’s actually the thickening of the epithelium that is the cause of the irregular shape,” he said.
Dr. Trattler said he doesn’t perform epithelial mapping routinely, as there is a lot of variability. “It’s not a perfect science yet because it can sometimes be difficult for the imaging technologies to differentiate between the tear film and the actual epithelium,” he explained.
Dr. Trattler also brought up the Artemis (ArcScan), a high-frequency ultrasound arc scanner. This technology uses a water bath and can differentiate between the epithelium and the tear film. Even with these other technologies, Dr. Trattler reiterated that topography is the most used and reliable for detecting irregular astigmatism.
Dr. Klyce and McDonald said, “Skiascopy and ray tracing add the ability to measure aberrations from the whole eye to determine whether the corneal endothelium or (more likely) the lens contribute significantly to ocular aberrations in addition to those due to the corneal surface. Corneal tomography with slit scanning instruments adds the ability to measure corneal endothelial optics and corneal thickness profiles. While corneal tomography provides these additional measurements and is less prone to error in highly aberrated corneas than corneal topographers, the latter remain the most accurate method to characterize the irregular astigmatism that has an early impact on visual acuity.”
Many treatments for causes of irregular astigmatism are covered by insurance, Dr. Trattler said, even if the initial topography that identified the astigmatism was not covered. “If a patient with a history of cataracts comes in with complaints of reduced vision, unless you perform topography/tomography and OCT of the macula, you may not identify other causes of the reduced vision, such as keratoconus (which can have a normal slit lamp exam when not too advanced), as well as vitreomacular traction syndrome. The advantage of performing topography and OCT prior to cataract surgery is that you identify these conditions prior to surgery.”
When it comes to cataract surgery planning for patients with irregular astigmatism, Dr. Trattler said patients with significant irregular astigmatism (even after ocular surface optimization, for example) are typically not candidates for a multifocal lens. He said a toric lens can be used if there is a “visible axis” and the degree of irregularity is mild. He said the Light Adjustable Lens (RxSight) or the IC-8 Apthera (Bausch + Lomb) are options as well.
“You might be able to use the IC-8 Apthera lens as a technology to help reduce the impact of the irregular astigmatism on vision. There are a lot of choices and options,” Dr. Trattler said.
Dr. Klyce and Dr. McDonald said it bears repeating that irregular astigmatism is defined and determined by evaluation of the HOAs measured from the reflections of Placido mires on the corneal surface. They added that some simpler HOAs have some optical properties that are useful for corneal diagnostics and IOL design.
“For example, coma is often associated with the inferior steepening seen in the topography of keratoconus. Spherical aberration is sometimes enhanced in laser refractive surgery to increase depth of focus in presbyopes,” they said. “However, the more complex HOAs generally combine to produce blur, halos, glare, starburst, or reduced contrast sensitivity that are uncorrectable with simple spherocylindrical optics. Topographic and wavefront-guided laser keratorefractive surgeries can reduce some of the HOAs but are generally most effective when treating the relatively simple HOAs (coma and spherical aberrations).”
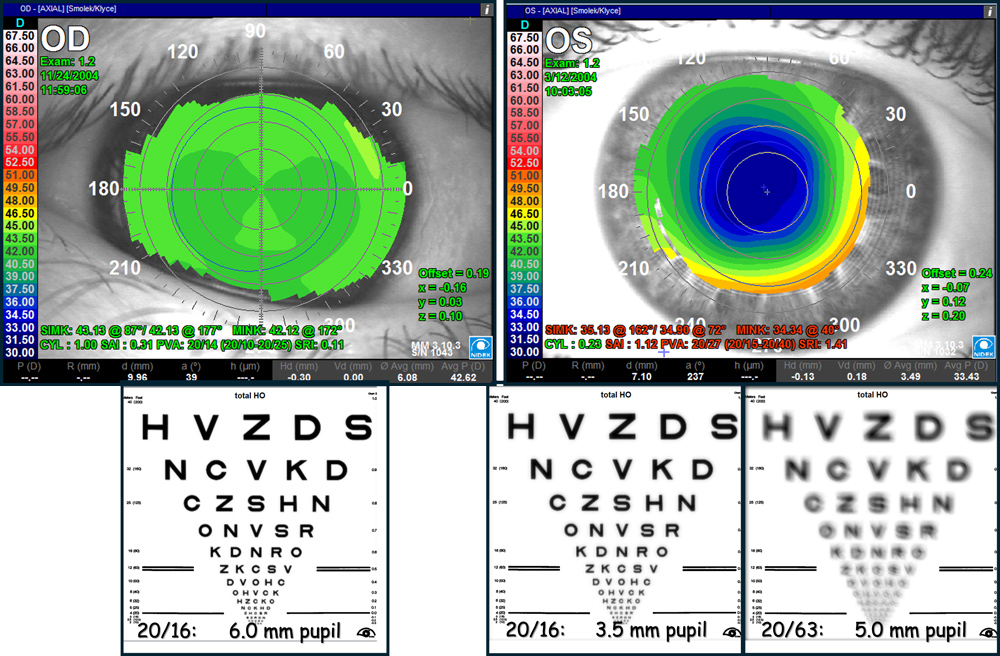
When it comes to IOL selection in the setting of HOAs, Dr. Klyce and Dr. McDonald said that a general “rule of thumb used by some physicians for IOL selection is to prefer a monofocal IOL rather than a premium channel extended focus or toric IOL, if the HOAs are greater than 0.5 µm RMS for a patient’s photopic pupil size.”
They said that quality of vision for an eye at different pupil sizes with an aberrated cornea can be obtained with Zernike terms and using optic calculations, assuming the rest of the eye is normal (Figure 2). “This approach can also be extended to address the impact of various IOL designs on vision obtainable for the individual patient if the optical design principles of an IOL are known,” they said.
Dr. Trattler’s final message was that he hopes topographic screening becomes more routine. He said it’s not uncommon that he discovers keratoconus, treatable with crosslinking, when patients have a screening topography, whether prior to cataract surgery, LASIK, pterygium surgery, or other procedures.
“The key issue is that we currently do not perform screening topographies on every single patient who comes to our office. Early keratoconus is often not detectable on slit lamp exam alone. If keratoconus is identified at an early stage, prior to vision loss, patients can be protected from progressive visual decline that may otherwise develop years later,” Dr. Trattler said.
About the sources
Stephen D. Klyce, PhD, FARVO
Adjunct Professor of Ophthalmology
Icahn School of Medicine at Mount Sinai
Port Washington, New York
Marguerite B. McDonald, MD, FACS
Clinical Professor of Ophthalmology
NYU Langone Medical Center
Clinical Professor of Ophthalmology
Tulane University Health Sciences Center
New Orleans, Louisiana
OCLI Vision
Oceanside, New York
William Trattler, MD
Director of Cornea
Center for Excellence in Eye Care
Miami, Florida
Reference
- Wilson SE, Klyce SD. Quantitative descriptors of corneal topography. A clinical study. Arch Ophthalmol. 1991;109:349–353.
Relevant disclosures
Klyce: Nidek
McDonald: Oculus
Trattler: ArcScan, Heidelberg, Oculus, Zeiss
Contact
Klyce: sklyce@klyce.com
McDonald: margueritemcdmd@aol.com
Trattler: wtrattler@gmail.com