Cornea
Spring 2025
by Liz Hillman
Editorial Co-Director
Three cornea specialists and one oculoplastics specialist agreed that in some cases, closing the eyelid with either a permanent or temporary tarsorrhaphy is among the best treatments for corneal healing; the procedure is, in many ways, “the cornea’s best friend.”
On the flip side, it’s not necessarily thought so by the patient—as Christopher Rapuano, MD, put it, “patients hate it”—and, as such, often requires trying multiple healing modalities prior to patients coming to terms with the procedure.
“The biggest problem with a tarsorrhaphy,” said Christopher R. Dermarkarian, MD, “is that you’re going to lose either some or all of the field of vision. … You’re limiting how much the patient can see. That is a big drawback to tarsorrhaphy—patients lose their peripheral vision or their entire field of vision.”
Dr. Rapuano, Dr. Dermarkarian, Kourtney Houser, MD, and D. Brian Kim, MD, gave their perspectives on when tarsorrhaphy is beneficial, different types of tarsorrhaphy, and how to help patients understand that while they might not want the procedure initially, it could, in many cases, speed healing for visual recovery and, in more severe cases, save their eye.



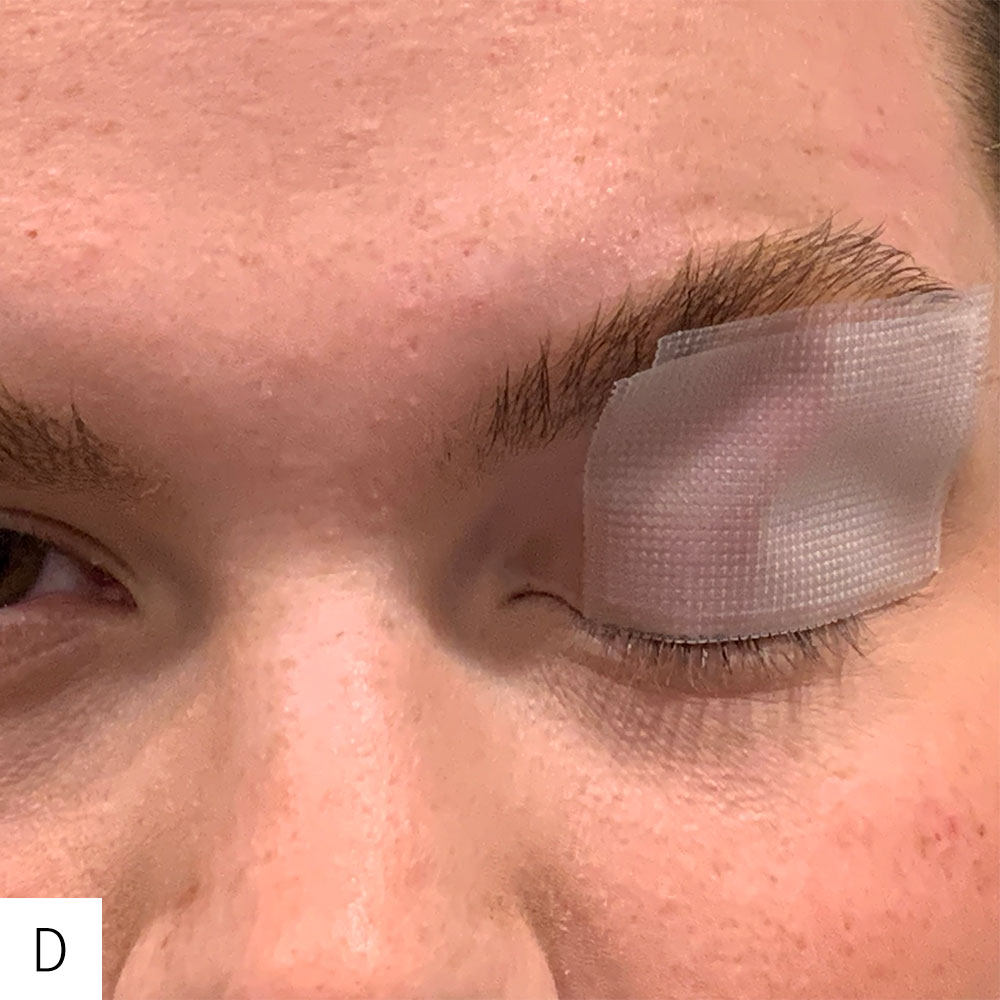

A. The upper eyelid skin is cleansed of any sebum with an alcohol wipe to maximize adhesiveness of the tape.
B. With the eyelid closed, the eyebrow is pulled upward in order to stretch the upper lid skin.
C. A 1 x 1.5-inch piece of 3M transpore water-resistant plastic tape is applied to the eyelid horizontally with the superior border of the tape just underneath the eyebrow.
D. Dr. Kim prefers to apply a second piece of tape to reinforce the splinting effect. The rigidity of the tape effectively creates a splint to maintain lid closure.
E. Observe the splinting effect of the tape with improved closure of the eyelid.
Source: D. Brian Kim, MD
Why tarsorrhaphy?
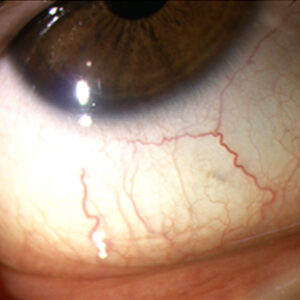
Dr. Kim shared that tarsorrhaphy protects the cornea because: 1) it limits corneal exposure to the environment, and 2) it limits corneal trauma from blinking. “The normal blink frequency is around 15–20 blinks per minute, and in the face of a persistent corneal epithelial defect or ulceration, the continual and repetitive movement of the eyelid over the cornea can undermine corneal healing,” he said.
Such persistent corneal epithelial defects, Dr. Kim continued, can be caused from numerous conditions, such as herpes keratitis, Bells palsy, contact lens overwear, and cicatricial lagophthalmos after eyelid surgery. Dr. Rapuano said he’ll also recommend a tarsorrhaphy after a corneal transplant when he has concerns about healing.
Dr. Kim said there are a variety of treatments that should be tried, in most cases, before tarsorrhaphy, including aggressive lubrication, punctal occlusion, therapeutic bandage contact lens, autologous serum, and/or amniotic membrane. “It is at the ophthalmologist’s discretion, but my general rule is if an epithelial defect persists for more than 7–10 days despite aggressive medical therapy, one should consider a tarsorrhaphy to reduce the risk for corneal haze or stromal melt. The use of oral doxycycline and vitamin C is also advised to minimize stromal complications,” he said.
Dr. Houser said she’ll outline what the options are leading up to this procedure—amniotic membrane, punctal plugs, artificial tears, Oxervate (cenegermin-bkbj, Dompe)—but she said that patients who have thin corneas near perforation or persistently diseased corneas despite multiple treatments would benefit from tarsorrhaphy sooner.
“If you could do a tarsorrhaphy for every epithelial defect, either medical or surgical, the corneas would absolutely love it,” Dr. Houser said. However, “[patients] don’t tend to like their eyelid being closed surgically or medically.”
Patient perceptions
Closing the eye, either partially or fully, temporarily or permanently, can be a “tough sell” for patients, Dr. Houser said, due to the functional and cosmetic issues it poses. As such, she said patients don’t usually come on board with the procedure until they’ve tried everything else.
“I think patients are usually not sold on it on the first visit unless they have something imminently vision threatening. So, if a patient comes in with a thin cornea with a risk of perforation, I may suggest that we do a tarsorrhaphy on my first visit seeing them. Most patients are amenable to a tarsorrhaphy if you explain to them that they have a vision- or eye-threatening condition.”
With some of the treatments tried prior to tarsorrhaphy requiring more frequent visits, Dr. Houser said some patients, depending on their living or medical condition, may opt for tarsorrhaphy initially as well.
Dr. Rapuano said it’s important preoperatively to tell the patient that this will be an uncomfortable procedure but that we’ll use a lot of medications to minimize the pain. This, he said, prepares the patient mentally for the procedure, so they “don’t think something horrible is happening” while it’s being performed. He said that while tarsorrhaphy can be a difficult choice for some patients, many, after having it done, say they wish they had done it earlier.
Types of tarsorrhaphy
All the surgeons interviewed for this article said standard suture tarsorrhaphy is within the purview of any ophthalmologist. Dr. Houser said she’ll perform some tarsorrhaphies herself and others she’ll refer to oculoplastics.
“Oculoplastic surgeons do eyelid surgery all the time. So especially if a patient has a concurrent ectropion or other eyelid issue, I think it’s good to have an oculoplastics colleague do it. But there are some patients in whom I want to do a tarsorrhaphy at the time of a high-risk corneal transplant or at the time of a transplant for perforation,” she said.
Depending on the type of tarsorrhaphy needed, Dr. Houser said they can be done medically, such as with Botox (onabotulinumtoxinA, AbbVie), or surgically. A temporary method that she uses in the operating room or clinic is a suture using a mattress stitch in a temporal position so the patient can still see out of the medial aspect of their eye. This also allows the physician to still examine the eye. Dr. Houser said for permanent tarsorrhaphy, she’ll often refer the patient to oculoplastics because that specialty is available to her, though, depending on logistics, she does perform them herself.
Dr. Rapuano said for a typical tarsorrhaphy, he uses black 4-0 silk on a double-armed needle and a foam bolster. He said he uses bolsters on the upper and lower lids, so the suture doesn’t “cheese-wire” through the skin over time. He’ll typically only close the outer third of the eyelid, but it closes about two-thirds of the eye, which facilitates healing and allows for examinations and for medications to be administered. He noted that even with permanent tarsorrhaphies, it can still be opened up later at the surgeon’s discretion. Some drawbacks to Botox tarsorrhaphy are that it doesn’t take effect immediately (often 1–3 days to kick in), and it’s unpredictable how long it will last, Dr. Rapuano said. He added that glue tarsorrhaphies can be problematic if the glue gets inside the eyelid and rubs against an already compromised cornea; it’s also unpredictable how long the glue will last.
Dr. Kim said since corneal fellowship, he has performed hundreds of surgical suture tarsorrhaphies (both temporary and permanent), but a few years ago, a representative from Bio-Tissue showed him a technique using a rigid piece of tape. “I have since given it the name tape tarsorrhaphy, then Dr. Michael Mimouni and the University of Toronto Cornea Department modified it to a more accurate description, which we now call tape-splint tarsorrhaphy.1 The tape-splint tarsorrhaphy has superseded my use of surgical temporary tarsorrhaphy, and it has been an invaluable tool because it is non-surgical, easily reversible, and the patient can apply it themselves,” he said.
Dr. Kim noted that tape tarsorrhaphy doesn’t work for all situations. “If there is a deep set orbit or excessively oily skin, it may not effectively splint the eyelid. There can also be intolerance due to contact dermatitis from the tape adhesive. Other times, a more permanent and aggressive method needs to be considered for chronic corneal exposure with a surgical suture tarsorrhaphy or a Gunderson flap, but I think from a patient informed consent perspective, the tape-splint tarsorrhaphy should be offered early in the process as a safe, non-surgical option.”
Dr. Kim said when performing a temporary suture tarsorrhaphy, he always uses bolsters to protect the eyelid skin under the bolster. He also suggested using a slip knot to titrate tension.
For permanent lateral tarsorrhaphy, Dr. Kim said his best pearl is when removing the anterior lamella of the eyelid margin, spare the lateral canthal area about 3–4 mm. “This is important because if and when you try and reverse the tarsorrhaphy, you will avoid rounding of the lateral canthus and achieve a much better cosmetic result,” he said.
Dr. Houser said she doesn’t use bolsters. “It’s a great procedure, with or without bolsters,” she said.
Dr. Dermarkarian, as an oculoplastics specialist, said permanent tarsorrhaphies are not a significant component of his practice, but he performs up to two a week. “I think anytime that people are asking for permanent tarsorrhaphy or a variation of the standard tarsorrhaphy, that is when they end up in my clinic for evaluation,” he said.
Dr. Dermarkarian discussed several “artistic variations” on the classic temporary suture tarsorrhaphy. He said glue tarsorrhaphies typically last for 5–7 days, and Botox tarsorrhaphies can cause complete ptosis that can last up to around 3 months. He said he doesn’t like the latter methodology because it is not as predictable, there could be hematoma formation in the eyelid or muscle, and there isn’t good control of the tarsorrhaphy timeline.
For permanent tarsorrhaphies, Dr. Dermarkarian places an incision through the gray line of the upper and lower eyelid margins and sutures the back part of the upper and lower eyelid together, then sutures the front part of the upper and lower eyelids together.
“In simple terms, the eyelid and eyelid margin are made up of two parts. There’s the skin and the muscle on the front side, and there’s the tarsus on the back side. The tarsus is like a form of cartilage. When you perform a permanent tarsorrhaphy, you want the upper eyelid tarsus to adhere to the lower eyelid tarsus, and you want to do the same for the skin and muscle of the upper and lower eyelid,” Dr. Dermarkarian said. “So medially you could do that, laterally you could do it, or you could do the entire eyelid depending on how much the eye needs to be closed.”
Dr. Dermarkarian said he thinks it’s important for patients to hear that even “permanent” tarsorrhaphies are reversible. “I always discuss with patients that it’s a great technique for healing, but if they hate it or if they’re miserable, we can easily take it apart in the clinic setting.”
Article Sidebar
Nandini Venkateswaran, MD, EyeWorld Cornea Editorial Board member, shared what she is excited for at the ASCRS Annual Meeting:
“The ASCRS Annual Meeting is one of my favorite meetings of the year! I always absorb so many wonderful clinical and surgical pearls and actively network with colleagues. I am very much looking forward to the meeting this year!”
About the physicians
Christopher R. Dermarkarian, MD
Assistant Professor of Ophthalmology
Oculofacial and Orbital Surgery
Duke University School of Medicine
Durham, North Carolina
Kourtney Houser, MD
Associate Professor of Ophthalmology
Duke University School of Medicine
Durham, North Carolina
D. Brian Kim, MD
Professional Eye Associates
Dalton, Georgia
Christopher Rapuano, MD
Chief of the Cornea Service
Wills Eye Hospital
Philadelphia, Pennsylvania
Reference
- Mimouni M, et al. Tape splint tarsorrhaphy for persistent corneal epithelial defects. Am J Ophthalmol. 2022;237:235–240.
Relevant disclosures
Dermarkarian: None
Houser: None
Kim: None
Rapuano: None
Contact
Dermarkarian: christopher.dermarkarian@duke.edu
Houser: Kourtney.houser@duke.edu
Kim: docdbk100@gmail.com
Rapuano: cjrapuano@willseye.org