Cornea: Beyond the routine
Fall 2025
by Ellen Stodola
Editorial Co-Director
Astigmatism, whether regular or irregular, is something that many ophthalmologists are familiar with. Amar Agarwal, MD, Jack Holladay, MD, MSEE, FACS, and Jack Parker, MD, PhD, discussed the issue and how to deal with it, particularly highlighting Dr. Agarwal’s pinhole pupilloplasty technique.
Astigmatism is the warpage of the front surface of the eye, Dr. Parker said. “The front surface of the eye should be round like a sphere, and if it’s not, if it’s warped, we call that astigmatism,” he said, noting that the astigmatism will either be regular or irregular.
Regular astigmatism is fully correctable with glasses or a soft contact lens, and this type is common. Occasionally, there will be irregular astigmatism, which is an abnormal shape of the cornea in which it is twisted or warped in a complex way; glasses and soft contact lenses won’t fix it.

Bottom left: Intraop, Purkinje image P1 in the center of the pupil
Top right: Intraop, microscope light switched off, visualization with endoillumination
Bottom right: Day 1 postop for a pinhole pupilloplasty, vision 6/9 N6
Source: Amar Agarwal, MD
There are certain diseases you can be born with or develop, like keratoconus, that may cause irregular astigmatism, Dr. Parker said. Additionally, things like trauma or prior surgery can cause a distortion of the surface of the eye.
These are aberrated corneas, Dr. Agarwal said, noting the term that he coined, “aberropia.”1 Aberropia is found in patients who have higher order aberrations, and there’s a problem with the clarity of their vision (resolution).
Dr. Parker said that topography or tomography are the most objective indicators of the shape of the cornea. But often, you don’t even need technology to diagnose irregular astigmatism. “You look at the eye, the best corrected vision is poor with glasses or contacts, and on exam, you see they have a big scar or the shape of the eye is twisted. These are usually grossly obvious things, which you can confirm with various imaging tools.” You can also see these distortions with the direct ophthalmoscope or retinoscope, which show scissoring of the light reflex indicating irregular astigmatism.
Meanwhile, Dr. Holladay described the value of topography and tomography, technologies that most surgeons have, in determining irregular astigmatism. He noted the axial and tangential maps, which show the front surface of the cornea. The more colors that you see in a topographic map, the more the irregularity; you’ll see patches of yellow, green, and blue, which are measures of irregularity that you can see on a topography, he said.
He also noted that physicians will want to pay attention to the RMS higher order aberration (HOA) values. In the cornea, we use the higher order aberrations, which are those irregularities on the surface, so they’re the high points and the low points, he said.
Irregular astigmatism is an older term for higher order aberrations, Dr. Holladay said. When wavefront came around, people stopped using irregular astigmatism because they could quantitate it and describe it with what are called Zernike coefficients. Now, that doesn’t make that much difference because what counts is how much the total irregularity is, and that’s where the RMS HOA value comes in.
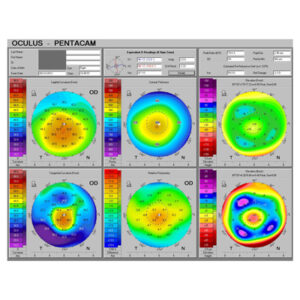
Dr. Holladay spoke about the “Holladay Report,” an interpretation guideline he put together for the Pentacam (Oculus). In it, he noted, “RMS HOA WE (6 mm), the RMS higher order aberration wavefront error over the 6 mm zone of the cornea, is a measure of corneal irregularity. A normal cornea has 0.37 μm. As the value increases above 0.66 μm, the image degradation from the cornea will become more noticeable, and above 1.00 μm, the patient will probably already have complaints about visual quality. The use of multifocal IOLs should be carefully considered with increasing amounts of corneal irregularity because it further reduces the contrast of the retinal image and glare and halos.”
Dr. Holladay described a study he did with Dr. Agarwal, showing that outcomes are related to the RMS HOA value because there are patients who have 2.0, 3.0, or 4.0 μm (10 times the normal value, which should be about 0.37), and those people are going to have bad vision. The effect of HOAs is directly proportional to the size of the pupil. A pinhole can help isolate these values to a small area and significantly reduce the effect of the HOAs.
The RMS HOA value is present on all topographers and tomographers, Dr. Holladay said. “Every single one has the RMS HOA 6 mm zone value because that’s a standard value that you need.” However, he noted that this value can be hard to find on some instruments. It’s always there, but it’s not always easy to find, and sometimes it requires calling the company to find out where it is, he said, adding that he wants to make physicians more aware of how to find this value on their own.
Conventionally, there have been two ways that irregular astigmatism could be treated, Dr. Parker said. The first way is with a hard contact lens, which vaults up above the surface of the eye and gives the eye a new shape. However, the problem with this is patients don’t generally want to wear these lenses all day. “It’s unpleasant at best and impossible for many people,” he said. The other way this can be treated is with a corneal transplant.
Pinhole pupilloplasty
Dr. Parker praised the development of the pinhole pupilloplasty technique by Dr. Agarwal, which utilizes the idea that through a small aperture, a pinhole-sized opening, stray rays of light can be filtered out, only permitting directly straight, focused light to impact the retina. “It’s an extremely simple, elegant way to solve a complex optical problem,” he said.

Source: Jack Holladay, MD
Dr. Parker noted that this technique has been slow to catch on, though he added that medicine is conservative, taking time to form a consensus on if a product or technique works.
Dr. Agarwal stressed the usefulness of using a pinhole pupilloplasty procedure to help these patients, adding that David F. Chang, MD, helped him come up with the term. You can make the pupil a specific size, he said, and the pinhole blocks rays of light that are creating aberrations. Only the central ray of light will go through, and patients see better immediately. Another advantage of pinhole pupilloplasty is that not only does the patient have good distance vision, but they see near without glasses.
Dr. Agarwal said the pinhole pupilloplasty procedure reduces the need for corneal transplants, which are limited by the availability of donor tissue. He noted the millions of people worldwide waiting for a corneal donor and the backlog associated with corneal transplantation. While pinhole pupilloplasty might not work in every corneal transplant case, it can help avoid a transplant in many scenarios. Pinhole pupilloplasty also has fewer complications, the patient recovers immediately, and it has helped to neutralize the astigmatism, he said.
Another advantage of this procedure is an anterior segment surgeon can perform the technique. Dr. Agarwal said that pinhole pupilloplasty may also be indicated for keratoconus, pellucid marginal degeneration, corneal scars, post-DALK, post-PK, etc.
One of the major benefits of the technique that he noted is that it neutralizes the astigmatism/HOAs without needing a nomogram.
Dr. Parker added that iris suturing is something of an art, and it’s not something everyone learns in training. Most general ophthalmologists, and even some corneal specialists, don’t do it or don’t do much of it, so there is an initial hurdle to overcome, operating on a delicate part of the eye.
Dr. Parker said there are drops that can constrict the pupil with pilocarpine. However, these can induce headaches, and he said he’s not sure if they really mimic the effect you get with a pinhole pupilloplasty because with pinhole pupilloplasty, you can titrate the size of the pupillary opening.
Dr. Holladay also noted drops using pilocarpine that can bring the pupil down to 1.0 mm or whatever size needed, based on the concentration of the drop. “The limitation with that is many times when you have a corneal scar, a penetrating keratoplasty, or irregularity in the cornea, that irregularity may be worse in the middle of the cornea,” he said. “So when you bring the pupil down, the pupil is right on that area of the greatest irregularity. With pinhole pupilloplasty, you can take this pinhole gauge that we have, and move it around to different positions, and you find the one where the cornea is clear and doesn’t have an irregularity. You can locate the pinhole wherever you want relative to the cornea, and with drops you can’t do that.”
Surgeons may also choose to use a pinhole IOL to help patients with irregular astigmatism, Dr. Agarwal said. The IC-8 Apthera (Bausch + Lomb) offers the pinhole technology. Dr. Agarwal said this is another good option, but he prefers the pinhole pupilloplasty procedure due to the ability to customize the location of the pinhole. “If the patient has a scar and I want to keep my pinhole pupil away from the scar, I can do this with pinhole pupilloplasty,” he said.
Additionally, he noted the lower cost of pinhole pupilloplasty and that it can be used for already pseudophakic patients. Pinhole pupilloplasty is also reversible. By doing a YAG laser, you can open the pinhole pupilloplasty or enlarge it if the patient complains of less illumination.
The customizable size with pinhole pupilloplasty is a big benefit, Dr. Agarwal said, adding that Dr. Holladay’s pinhole device has helped enable the ability for patients to choose the size pupil that will work for them.
“You can’t get a cornea to be as perfect as the original when you do a penetrating keratoplasty, but if their lens is clear, if they have an intraocular lens, this little gauge allows us to put that in front of the patient, and depending upon the amount of irregularity, you can find out which pinhole will give them the best vision,” Dr. Holladay said.
In someone who has a mild amount of irregularity, Dr. Holladay said they may get up to a 2.5-mm pupil and see 20/20. If someone has, for example, an injury from a piece of metal that hit the cornea with a bad irregularity, they may need a smaller pupil. They could end up with a 0.5, 1.0, or 1.5 mm, he said. “This little pinhole allows us to determine the size of the pinhole we want to achieve at surgery.”
Pinhole pupilloplasty is beginning to catch on, Dr. Agarwal said, noting that physicians in India, the U.S., Russia, Egypt, and other countries are performing it. Dr. Holladay finds the technique to be more common internationally, though he predicted it will increase in frequency and in prevalence over time in the U.S.
While he said it can also be used for corneal transplantation, he noted that the U.S. is less likely to have conditions like trachoma and other diseases that may be more prevalent in other parts of the world.
One of the limitations in using a pupilloplasty, Dr. Holladay said, is that once you make the pupil 1.0 mm, your ability to see the peripheral retina goes away. “When we do normal eye exams, the first thing we do is dilate the pupil up to 10 so we can see out in the periphery and make sure the patient has no retinal tears, holes, or anything that needs treatment, and once you make that pupil 1.0, all that goes away,” he said.
One scenario where he finds this being used the most is in someone who’s had cataract surgery who has a clear lens but doesn’t see well because the cornea is the limiting factor. These patients are prime candidates for pupilloplasty because you can locate the pupilloplasty where you want it and make it the size that you need, using the gauge for precision before you ever go to surgery, Dr. Holladay said.
Dr. Parker noted that he wouldn’t generally use pinhole pupilloplasty on phakic patients, though you could do it after or at the same time as cataract surgery. “There’s a risk of damaging the patient’s natural lens because you’re sewing on top of it, and at some point, you’ll have to reverse the pupilloplasty to fix that patient’s cataract in the future.” So it’s better to remove the cataract before or at the time of pupilloplasty.
The biggest fear that eye doctors have is visibility to the back of eye, Dr. Parker said. If you make the pupil smaller, you may not be able to dilate the patient anymore, and that could be a concern. However, he noted that modern fundus photography instruments help make this less of an issue.
Article sidebar
Kevin Miller, MD, EyeWorld Cataract Editorial Board member, shared how he goes “beyond the routine”:

“Many people read our electronic medical record (EMR) chart notes—fellow ophthalmologists, internists, other physicians, payers, even patients—after an office visit. To avoid confusion, we do not use any abbreviations or acronyms such as TFBUT (for tear film break-up time) anywhere in our notes. Instead, we spell everything out. Fortunately for us, our EMR has a customizable dictionary that allows us to automatically turn any abbreviation or acronym we have created into spelled-out text. This is especially useful when an abbreviation such as SLE can be interpreted two different ways, such as slit lamp examination or systemic lupus erythematosus.”
About the physicians
Amar Agarwal, MD
Chairman
Dr. Agarwal’s Group of Eye Hospitals
Chennai, India
Jack Holladay, MD, MSEE, FACS
Clinical Professor
Department of Ophthalmology
Baylor College of Medicine
Houston, Texas
Jack Parker, MD, PhD
Parker Cornea
Vestavia Hills, Alabama
Reference
- Agarwal A, et al. Aberropia: a new refractive entity. J Cataract Refract Surg. 2007;33:1835–1836.
Relevant disclosures
Agarwal: None
Holladay: None
Parker: None
Contact
Agarwal: aehl19c@gmail.com
Holladay: holladay@docholladay.com
Parker: jack.parker@gmail.com