November 2013
Cover Feature: Corneal crosslinking
by Vanessa Caceres
EyeWorld Contributing Writer
FAQs your patients may have
Corneal collagen crosslinking (CXL) is known as a generally successful procedure for patients with corneal ectasia, but naturally, patients come to their surgeons with a host of questions. How soon can I wear contact lenses or glasses again? What complications might occur? When will my vision stabilize after crosslinking? Could my keratoconus symptoms return?
EyeWorld consulted with some CXL pros to find out how they typically handle patients’ most common questions.

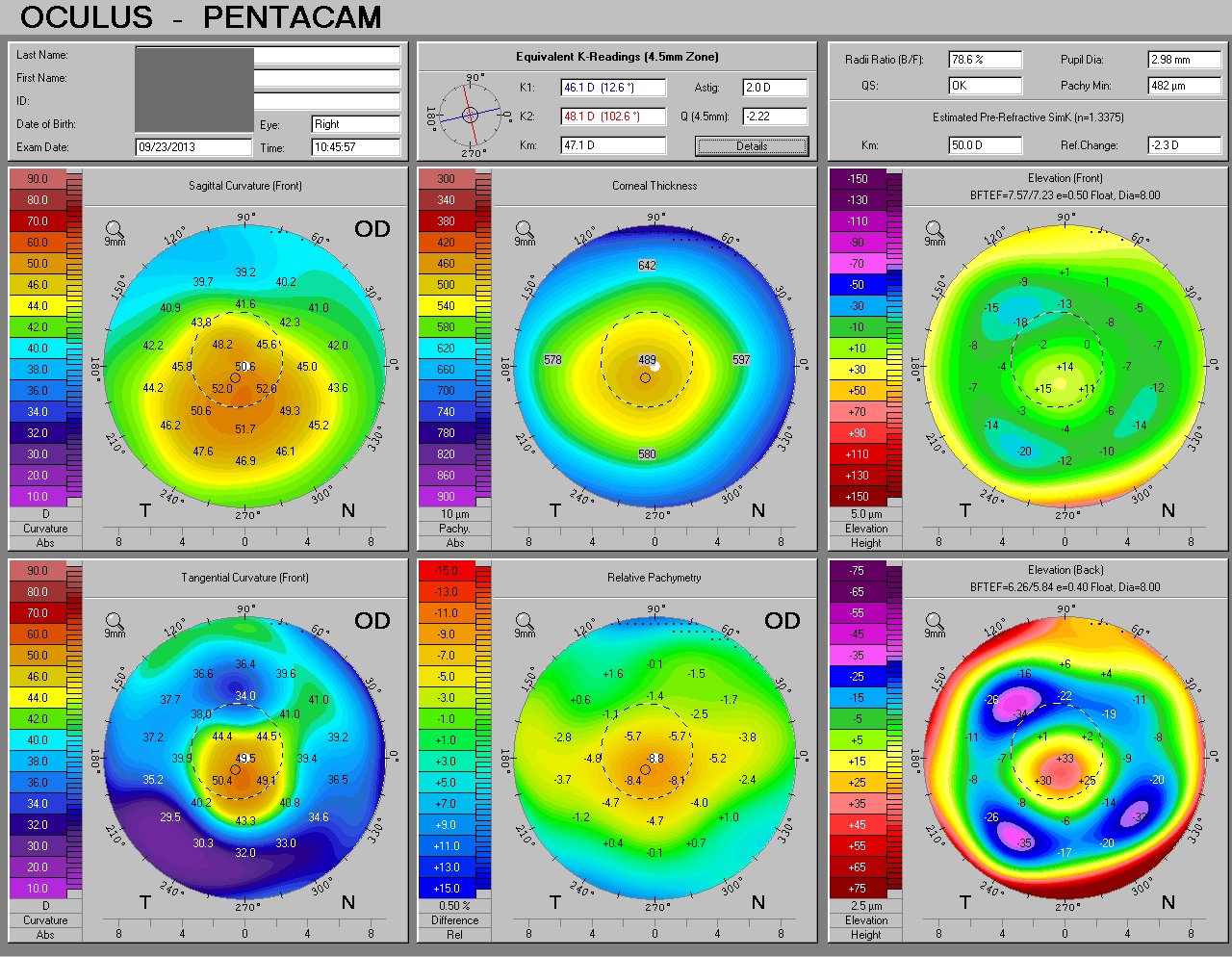
Source (all): Sumit Garg, MD
1. When can I wear contact lenses or glasses again?
“I generally recommend my patients stay out of contact lenses for a few weeks postoperatively,” said Sumit (Sam) Garg, MD, vice chair of clinical ophthalmology, and assistant professor, cataract, corneal and refractive surgery, Gavin Herbert Eye Institute, University of California, Irvine. “I try to have them aggressively lubricate the surface and allow for the epithelium to return to normal prior to recommending contact lenses. Aggressive lubrication helps smooth out the epithelium, therefore stabilizing vision.”
Roberto Pinelli, MD, scientific director, Istituto Laser Microchirurgia Oculare (ILMO), Crystal Palace, Brescia, Italy, recommends patients wait for a month after CXL before they wear their contact lenses again.
2. When will my vision stabilize again?
Can there be fluctuations? Fluctuations do indeed occur, although they generally last only a couple of months. Patients are usually able to return to work or school in a day or two, said Michael B. Raizman, MD, Ophthalmic Consultants of Boston, director, cornea and cataract service, New England Eye Center, and associate professor of ophthalmology, Tufts University School of Medicine, Boston. After that, he finds patients may have blurry vision for a few days to one week. “At that point, the vision is usually close to baseline, and the existing spectacles will typically suffice.”
Over the first year, the cornea typically steepens at first and then flattens, said Dr. Raizman. “The chief purpose of crosslinking is to stabilize the cornea to prevent progression, but many patients actually have some improvement in vision,” he said.
“With the epithelium-off technique, visual fluctuations are very common in the initial healing period,” Dr. Garg said. “Just as in photorefractive keratectomy, it takes time for the epithelium to heal and normalize over the cornea surface.”
3. When should I get my prescription changed?
“Patients need to understand that crosslinking can cause a change in their keratometry the first few months after treatment, and this means their prescription may also change,” said Dr. Garg.
Ultimately, most surgeons recommend that patients wait until a couple of months after treatment to ensure a stable refraction. “We see a stability of refraction at three to six months,” said Dr. Pinelli.
4. What types of complications should I be aware of?
Although it’s not a complication per se, initial discomfort is common. Dr. Raizman will help ease patients’ discomfort in the immediate postop period with a bandage contact lens and the use of drops and oral analgesics.
However, beyond that, complications are not seen often, he said. “The cornea always has mild haze, but this affects the vision only rarely,” said Dr. Raizman. “If the vision is reduced by haze, this almost always improves on its own over a few months.”
One rare complication is infection, said Dr. Raizman. “That can be avoided in almost all cases through the use of topical antibiotics after surgery and careful observation at postoperative visits.”
The CXL procedure itself is very safe, said Dr. Garg, although complications such as infectious keratitis, sterile infiltrates, reactivation of herpes simplex keratitis, and slow epithelial healing can occur.
David Rootman, MD, professor of medicine, University of Toronto, and director, Yonge Eglinton Laser Eye Centre, Toronto, has used the patients’ own serum tears and amniotic membrane transplantation as biologic treatments for patients with slow epithelial healing.
5. What are the symptoms of progressive keratoconus?
“Crosslinking is not meant to make keratoconus go away,” Dr. Rootman said. Instead, it is meant to stop or slow down disease progression. This is why patients should know about progressive keratoconus symptoms, such as vision deterioration with increased astigmatism, a change in prescription, contact lens intolerance, and overall poorer visual distortion and vision function. The standard follow-ups at six and 12 months will help verify that keratoconus progression slowed, Dr. Rootman said.
Epi-on and epi-off
The surgeons interviewed by EyeWorld support their respective surgical approaches as a way to avoid unnecessary complications. Drs. Garg, Raizman, and Rootman use the epithelium-off approach (also called epi-off). “The vast majority of cases and almost all the medical literature relates to treatment with the epithelium off,” said Dr. Raizman. “Recent efforts to achieve effective crosslinking without removing the epithelium show that this will likely be successful in the future, but more clinical trials are required to determine the best approach.”
Higher light energy and enhanced riboflavin delivery to the corneal stroma will be needed to achieve the optimal results obtained with epi-off, Dr. Raizman added.
“I have seen several unfortunate young patients who had crosslinking without epithelial removal and then had rapid ongoing progression of their keratoconus. This is almost never seen with epithelium-off crosslinking,” Dr. Raizman said.
Dr. Pinelli performs the transepithelial technique, which allows CXL to be performed more quickly and does not involve removal of the epithelium. Dr. Pinelli uses the transepithelial technique with ParaCel (Avedro, Waltham, Mass.).
Editors’ note
Dr. Garg has financial interests with Abbott Medical Optics (Santa Ana, Calif.). Dr. Pinelli has financial interests with Avedro. Dr. Raizman has financial interests with Alcon (Fort Worth, Texas), Allergan (Irvine, Calif.), Avedro, and Bausch + Lomb (Rochester, N.Y.). Dr. Rootman has no financial interests related to this article.
Contact information
Garg: gargs@uci.edu
Pinelli: pinelli@ilmo.it
Raizman: mbraizman@eyeboston.com
Rootman: d.rootman@utoronto.ca



