Refractive: Strike!
Fall 2024
by Liz Hillman
Editorial Co-Director
Whether you’re doing laser vision correction or refractive cataract surgery with an advanced-technology IOL, among the many measurements that influence procedural decisions are higher order aberrations (HOAs).
“Corneal HOAs should be assessed during the preoperative evaluation for all refractive and cataract surgeries as a standard practice to inform surgical planning,” said Brian Armstrong, MD. “Missing preoperative HOAs can lead to suboptimal outcomes, including residual refractive error, poor visual quality, and visually significant dysphotopsias. Postoperative management of a dissatisfied patient may involve IOL exchange or laser vision enhancement to address these issues.”
While whole chapters have been written on the topic of HOAs, Dr. Armstrong, along with Karolinne Maia Rocha, MD, PhD, and Damien Gatinel, MD, PhD, discussed measuring and quantifying HOAs, their impact on IOL selection for cataract surgery, procedure and candidate selection for corneal refractive surgery, and some of their eccentricities.
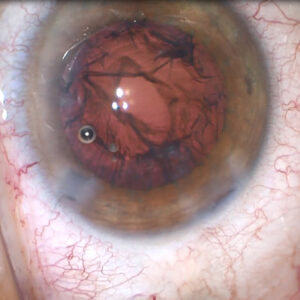
Dr. Rocha said that HOAs and light scatter can be induced by various sources: dry eye, age-related cataract, posterior capsular opacification, vitreous floaters, keratoconus, and too small of an optical zone or decentered ablations post-corneal refractive surgery. No eye is perfect, she said, though patients are more likely to tolerate/compensate for HOAs that they’re “born with” compared to those that are induced.

Source: Karolinne Rocha, MD, PhD
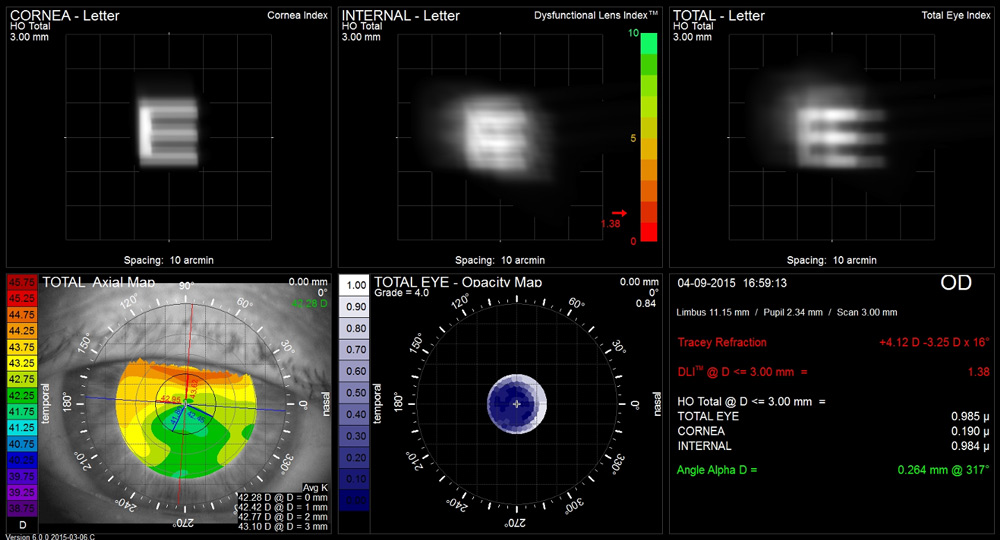
Source: Karolinne Rocha, MD, PhD
How to measure and quantify
There are several technologies to identify and quantify HOAs. Dr. Rocha spoke about devices that use Shack-Hartmann wavefront sensors, ray tracing, double-pass sciascopy, OCTs, and Scheimpflug tomography. She said some devices measure the entire eye’s aberration profile, the corneal HOAs, while others measure the cornea and the whole eye’s aberrations.
Dr. Rocha also talked about adaptive optics technology, which is not commercially available, that simulates the patient’s vision when correcting and adding aberrations, and how much they can tolerate. Dr. Rocha shared two studies with an adaptive optics visual simulator showing that the patients’ HOAs could be measured and corrected by the simulator.1,2 One of these studies suggested that “adaptive optics technology may be of clinical benefit when counseling patients with highly aberrated eyes regarding their maximum subjective potential for vision correction.”2
Dr. Armstrong said corneal HOAs are clinically assessed with advanced tomography devices like the Pentacam (Oculus), Galilei (Ziemer), and MS-39 anterior segment OCT (CSO).
“These devices provide a detailed analysis of corneal HOAs by evaluating both anterior and posterior corneal surfaces, as well as pachymetry and densitometry data,” he said. “They provide a quantification and stratification of HOAs. Placido disc-based topography is a more affordable method to quantify HOAs, though it does not provide data on posterior or total corneal HOAs. For the most cost-effective approach, one can infer increased HOAs from the reflection of irregular mires on a keratometer and keratoscope or scissor reflex seen with a retinoscope. While these tools offer insights into corneal irregularities, they lack the ability to quantify HOAs.”
Patient perspective
Putting a number on HOAs is one thing, but understanding the patient’s perception of them is important as well.
“HOAs can diminish best spectacle corrected visual acuity and cause symptoms like glare and halos around lights, particularly in low light conditions. The impact is often more pronounced in patients with larger pupil sizes. You can determine the impact on vision of corneal HOAs by doing a diagnostic hard contact lens over refraction,” Dr. Armstrong said. “Usually, the difference in best spectacle corrected vision with and without a hard contact lens can be attributed to HOAs. Clinically, we may perform contrast sensitivity testing to gauge the subjective impact of HOAs, which can be reduced in patients with increased HOAs. Wavefront aberrometry is another tool that provides a comprehensive evaluation of total eye HOAs, offering both quantitative data and visual simulations for patient education. In our practice, we use a newer aberrometry device called the Osiris [CSO], which integrates with tomographic data from the MS-39 anterior segment OCT to provide a more comprehensive assessment of an eye.”
Dr. Armstrong said that while there is no data-driven link between a person’s personality and their subjective perception of HOAs, the stereotypical “type A” personality is generally more likely to be bothered by visual quality issues related to HOAs.
“It is important for the ophthalmologist to identify patients who prioritize visual quality over spectacle independence as we decide upon an IOL to implant,” he said. “Each surgeon should develop a way to tease out that information, either by way of questionnaire or during face-to-face consultation. If you suspect the patient to be ‘type A,’ you should plan to do your best to address preexisting HOAs and possibly avoid presbyopia-correcting diffractive IOL implantation.”
HOAs informing IOL selection
Dr. Armstrong said he’ll tailor his IOL selection to the patient’s corneal HOAs, avoiding presbyopia-correcting IOLs that use diffractive optics if the abnormal HOAs cannot be addressed preoperatively.
“Monofocal IOLs are a safer option because they are less affected by HOAs,” he said. “Pinhole IOLs can partially neutralize the visual impact of corneal HOAs. … Normal spherical aberration of the cornea is about 0.3 μm for a 6-mm pupil size, thus most common IOLs have a negative spherical aberration of about –0.2 μm (matching that of the natural crystalline lens). However, in patients with abnormal levels of spherical aberration (>±0.5 μm), we should consider picking an IOL that shifts the spherical aberration of the eye closer to zero. We have an array of IOLs, some of which have negative, neutral, and positive spherical aberration, and we should do our best to utilize the right IOL to achieve the best possible visual outcome.”
Dr. Rocha offered a similar perspective, discussing the different enhanced monofocal IOL options that offer customization for patients with HOAs.
“You can even customize with the new generation of monofocal IOLs or enhanced monofocal IOLs; we have a lot of options. Some are aberration-free. Some come with positive or negative spherical aberration. I think the rule is you should not end up with more than 0.4 μm of spherical aberration after implanting that IOL,” she said.
Dr. Gatinel said to focus on corneal aberrations in this case because any preop aberrations from the lens will be removed in cataract surgery. “In this situation, you need to direct the corneal wavefront,” he said, adding that research should be conducted to understand the interactions between the IOL options and different corneal aberrations to “cherry pick the one that is most relevant for the patient.”
HOAs and refractive surgery
If a patient is seeking refractive surgery, not yet needing cataract surgery, and has HOAs, Dr. Gatinel said he’ll first tell patients to stop rubbing their eyes. Once it seems like they’ve understood the importance of this and they don’t progress, he finds wavefront-guided PRK to be the best option to improve the corneal shape. If you’re confident they won’t rub their eyes in the future, and the corneal topography shows moderate abnormalities, LASIK could be an option. He added that he would avoid premium lens implantation after lenticular extraction for patients with elevated and/or symptomatic HOAs. Dr. Rocha, in a presentation, offered several pearls for managing HOAs in the setting of corneal refractive surgery.
- Make sure maps are reproducible and verify long-term refractive stability.
- Compare the wavefront refraction with the manifest and cycloplegic refractions and the topographic maps with wavefront aberrations.
- For enhancements, use SD-OCT to determine whether LASIK or PRK is better (PRK with mitomycin-C for cases with thin pachymetry and thick flaps; don’t relift flaps if you can’t identify the thickness profile).
- Recognize that the ablation depth for a specific refraction increases with the magnitude of aberrations, leading to overcorrection.
- Discuss with the patient that this might be a two-step treatment due to the potential shift in lower order aberrations when correcting HOAs.
Dr. Rocha’s presentation also emphasized that management of HOAs is technology dependent. Not all platforms perform the same, and HOA treatment is subject to technology limitations.
A word about Zernike
Dr. Gatinel spoke at length about Zernike polynomials and how they may not always accurately represent the visual quality because they sometimes misrepresent defocus and other aberrations.
Dr. Gatinel published an “alternative wavefront reconstruction method” in 2020, proposing that “some of the inherent limitations of Zernike polynomials in clinical ophthalmic application can be solved by a novel set of polynomials forming an alternative higher order basis. The new basis provides a clear separation between modes containing lower order terms versus higher order terms and offers clinicians a more clinically realistic wavefront analysis.”1
In his interview with EyeWorld, Dr. Gatinel said that the real defocus people select to correct with spectacles is not the Zernike defocus. “Zernike defocus is in displays where you would say that’s the defocus, but this is particular in eyes with a lot of spherical aberrations, which are eyes with a lot of problems. This Zernike defocus is not the refractive defocus,” he said. In addition, the retinal image simulations and related metrics for HOAs using Zernike decomposition are not always clinically relevant as some low order aberrations such as defocus or astigmatism are embedded in the expression of some higher order Zernike modes.
Reference
- Gatinel D, et al. An alternative wavefront reconstruction method for human eyes. J Refract Surg. 2020;36:74–81.
About the physicians
Brian Armstrong, MD
Associate Professor of Ophthalmology
Director of Cornea and Refractive Surgery
University of Nebraska Medical Center
Truhlsen Eye Institute
Omaha, Nebraska
Damien Gatinel, MD, PhD
Head of the Anterior and Refractive Surgery Department
Rothschild Foundation
Paris, France
Karolinne Maia Rocha, MD, PhD
Professor of Ophthalmology
Medical University of South Carolina
Storm Eye Institute
Charleston, South Carolina
References
- Rocha KM, et al. Effects of Zernike wavefront aberrations on visual acuity measured using electromagnetic adaptive optics technology. J Refract Surg. 2007;23:953–959.
- Rocha KM, et al. Enhanced visual acuity and image perception following correction of highly aberrated eyes using an adaptive optics visual simulator. J Refract Surg. 2010;26:52–56.
Relevant disclosures
Armstrong: None
Gatinel: Alcon, BVI, Heidelberg Engineering, Moria, Nidek, Rayner
Rocha: Alcon, Allergan, Bausch + Lomb, Johnson & Johnson Vision
Contact
Armstrong: brarmstrong@unmc.edu
Gatinel: gatinel@gmail.com
Rocha: karolinnemaia@gmail.com